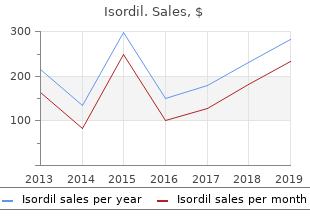
Isordil
"Best isordil 10mg, medicine and science in sports and exercise".
By: T. Frillock, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Assistant Professor, Sam Houston State University College of Osteopathic Medicine
Diagnosing idiopathic regular-stress hydrocephalus medicine 50 years ago proven isordil 10 mg, Neurosurgery 2005;fifty seven (3 Suppl): S2-4-S2-16 symptoms 6dpiui proven isordil 10mg. Infrequently carried out studies in nuclear medicine: Part 2 treatment centers in mn order 10mg isordil, J Nucl Med Technol 2009 Mar; 37: 1-13 medicine 5325 generic 10 mg isordil. Patient with a shunt (ventriculo-peritoneal, ventricular-pleural or 3 ventricular venous) that may be blocked [Certify 78645] References: 1. American College of Radiology Appropriateness Criteria � Dementia and Movement Disorders. Diagnosing idiopathic regular-stress hydrocephalus, Neurosurgery, 2005; fifty seven:S2-4-S2-16. Infrequently carried out studies in nuclear medicine: Part 2, J of Nuclear Medicine Technology, 2008; 36:132-143. Mostly pediatric sufferers with prior pyelonephritis inflicting scarring, or known ureteral reflux that might result in pyelonephritis and scarring. Acute pyelonephritis with bacteriuria for kids age 2 months to 3 years could also be carried out 4-6 months after the infection to 1-4 detect scarring V. Society of Nuclear Medicine, Procedure Guideline for Renal Cortical Scintigraphy in Children, version 3. American Academy of Pediatrics, Committee on Quality Improvement, Subcommittee on Urinary Tract Infection. Practice parameter: the diagnosis, therapy, and evaluation of the initial urinary tract infection in febrile infants and younger youngsters, Pediatrics, 1999, 103:843-852. Society of Nuclear Medicine Procedure Guideline for Renal Cortical Scintigraphy in Children, version 3. Refractoriness to aggressive medical remedy (usually failure to respond to 3 drug remedy) B. Suspected obstructive uropathy (78708 or 78709 renal scan with pharmacologic intervention) V. American College of Radiology Appropriateness Criteria � Renovascular Hypertension. European Association of Urology, European Society for Paediatric Urology, Guidelines on Paediatric Urology, 2009. Society of Nuclear Medicine Procedure guideline for diagnosis of renovascular hypertension, version 3. Expert Panel on Urologic Imaging, American College of Radiology Appropriateness Criteria � Renal Failure. Urinary tract infection in a baby with poor response to 48 hours of antibiotics with urinary retention, elevated creatinine or 1 recurrent febrile urinary tract infections References: 1. Suspicion of urinary retention with ultrasound not diagnostic [One of the following] A. Society of Nuclear Medicine, Procedure Guideline for Radionuclide Cystography in Children, version 3. Paediatric Committee of the European Association of Nuclear Medicine, Guidelines for direct radionuclide cystography in youngsters. Paediatric Committee of the European Association of Nuclear Medicine, Guidelines for direct radionuclide cystography in youngsters. American College of Radiology Appropriateness Criteria � Acute Onset of Scrotal Pain�without Trauma, without Antecedent Mass. Patients with a historical past of prostate carcinoma treated with radiation or seed implantation, etc. The position of imaging with 111In-ibritumomab tiuxetan within the ibritumomab tiuxetan (Zevalin) regimen: outcomes from a Zevalin Imaging Registry, J Nucl Med, 2005; forty six:1812-1818. In the presence of orthopedic hardware or prosthesis, regular bone marrow is disrupted and displaced, making interpretations difficult in these areas. Comparison of 111In leukocyte localization with 99mTc-sulfur colloid uptake using mixed or sequential 111In-leukocyte/99mTc colloid photographs is often essential. A white-cell scan should be accompanied by a bone marrow scan using 99mTc sulfur colloid carried out either collectively or sequentially. Society of Nuclear Medicine Procedure Guideline for 111In-Leukocyte Scintigraphy for suspected infection /inflammation, Version 3. Restaging during chemotherapy in a member with known metastases, if standard imaging is equivocal or inconclusive C. Surveillance of an asymptomatic individual not on therapy and having no new signs or symptoms regarding for recurrence 11 V. For monitoring response to remedy until standard imaging is inconclusive Page 857 of 885 5. Restaging for suspected recurrence of Merkel Cell Carcinoma, when standard imaging is inconclusive or negative for metastases C. Surveillance of an asymptomatic individual not on therapy and having no new signs or symptoms regarding for recurrence Page 858 of 885 29-30 X. Initial staging if standard imaging exhibits no proof of metastatic illness B. Patient is surgical salvage candidate for recurrence and no metastatic illness is famous on standard imaging C. Isolated metastatic lesion famous on standard imaging and patient is a candidate for aggressive surgical resection or native therapy of metastases with a curative intent 2. Soft tissue sarcoma (extremity, head/neck, abdominopelvic, sixty one-66 retroperitoneal and gastrointestinal stromal tumors) A. For planning neoadjuvant remedy previous to surgical resection of tumors >3 cm on standard imaging 4. To verify oligometastatic illness previous to surgical resection with curative intent 4. Benign bone tumors such as osteochondroma, chondroblastoma, desmoplastic fibroma, osteoid osteoma, enchondroma and large cell tumors of the bone 2. Suspected Richter�s transformation from a low grade lymphoma to a extra aggressive kind when any one of the following is current: 1. Evaluation of chronic lymphocytic leukemia/small lymphocytic lymphoma until Richter�s transformation is suspected 3. Surveillance of an asymptomatic individual not on therapy and having no new signs or symptoms regarding for recurrence 6. Restaging after completion of major radiation with/without chemotherapy if the patient is a surgical salvage candidate C. Non-epithelial ovarian cancers � germ cell tumors, sex wire stromal (granulosa cell) tumors and ovarian tumors of low malignant potential 2. Suspected recurrence with rising tumor markers and negative or inconclusive standard imaging B. Non-seminomatous germ cell tumors, sex wire stromal tumors (Sertoli Leydig cell tumors) 2. Clinical or laboratory findings suggesting benign etiology, and no historical past of malignancy 1. If no adjustments at 3 months, 2 further observe-up scans (at 6 months and one year) could be permitted. Takayasu arteritis Any of the following are indicated for evaluation of Takayasu arteritis: A. Patients with aggressive illness being treated with systemic remedy can have imaging (see specific sections for details regarding modality and contrast stage) permitted for therapy response every 3 months during active therapy References: 1. American College of Radiology Appropriateness Criteria � Radiographically Detected Solitary Pulmonary Nodule. American College of Radiology Appropriateness Criteria � Non-Invasive Clinical Staging of Bronchogenic Carcinoma. Prospective comparison of computed tomography, diffusion-weighted magnetic resonance imaging and [11C]choline positron emission tomography/computer tomography for preoperative lymph node stating in prostate cancer sufferers. Dimopoulos M, Terpos E, Comenzo Rl et al, International myeloma working group consensus statement and tips regarding the present position of imaging methods within the diagnosis and monitoring of a number of myeloma, Leukemia 2009;23:1545-1556. Category 4B is intended to direct the individual out of screening and into a diagnosis primarily based on a bigger, growing or more and more suspicious nodule. Catching: Along with throwing, catching is among the two most important skills in Ultimate Frisbee.
Diseases
- Gliosarcoma
- Cardiomyopathy, fatal fetal, due to myocardial calcification
- Dermochondrocorneal dystrophy of Fran?ois
- Atrophy
- Corneal cerebellar syndrome
- Infundibulopelvic stenosis multicystic kidney
- Long QT syndrome type 2
Glu cocor t icoid s (steroid s) h ave been sh ow n t o h ave n o ben eficial e ect on survival rate or neuro logical restoration rate after cardiac arrest medicine 74 generic isordil 10mg. In: Emergency Room Managem ent of Tr a u m a t ic Tr a n s t e n t o r ia l He r n ia t io n symptoms mercury poisoning generic isordil 10 mg. He a d In ju r ie s in Ch ild r e n Un d e r ninety six 36 Months of Age: Demography and Outcome medicine education safe isordil 10mg. The Diagnosis of Stupor and Syst e m a t ic Re vie w o f Ea r ly Pr e d ict ion of Po or Ou t Co m a medicine you can overdose on buy isordil 10mg. Acute Brain Herniation: A Revised Con cocorticoid Treatment Does Not Improve Neurologi cept. Un ifo r m d e t e r m in a t io n o f d e a t h a c t, 1 9 8 0 (v e r b a t im q u o t e) �An in d ivid u a l w h o h a s s u s t a in e d e it h e r 1. A d e t e r m in a t io n o f d e a t h m u s t b e m a d e wit h a c ce p t e d m e d ic a l s t a n d a r d s. Fo r in d ivid u a ls < 5 ye a r s a ge, s e e Br a in d e a t h in ch ild r e n (p. When the cause of dying is aside from pure causes the Medical Examiner or Coroner (rely ing on the authority in your jurisdiction) w sick be contacted per hospital coverage. Ke y p o i n t: Cr i t e r ia s h o w n b e l o w m a y b e u s e d t o d e t e r m i n e t h e c l i n i c a l a b s e n ce o f b r a i n a n d brainstem operate. Then to be sure that the whole cessation of mind operate is irreversible, the clini cian m ust take into consideration the cause of the absence, and exclude conditions that may m im ic the clinical look of mind dying. This might require ancillary confirmatory checks and observation for a p e r iod of t im. Waiting durations: There is insu cient evidence to support a particular observation interval to guarantee three that the cessation of neurologic operate is irreversible. Th is r e q u ir e s t h a t t h e d e t e r m in a t io n o f mind dying take into consideration the entire available data and circumstances. Absence of brainstem reflexes: a) ocular examination: fixed pupils: no response to brilliant mild (caution after resuscitation: see beneath). Wait no less than 1minute for response,and 5minbeforetestingtheoppositeside(to prevent cancellation of opposing response) b) absent oropharyngeal reflex (gag) to stimulation of posterior pharynx c) no cough response to bronchial suctioning 2. If complex built-in motor actions occur, it is suggested that 12 affirm atory testing be perform ed previous to pronouncem ent of mind dying 4. Below this temp, pupils may be fixed and 13 14 dilated, respirations may be di cult to detect, and restoration is feasible b) no evidence of remediable exogenous or endogenous intoxication, together with drug or metabol ic (blood alcohol level ought to be < 0. Pseudocholinesterase deficiency is current in 1/3000 sufferers which may trigger succinycholine to last up to 8 hours (as an alternative of 5 mins). Loss of>45%of circu lating blood volum e can produce lethargy d) instantly submit-resuscitation: shock or anoxia might trigger fixed and dilated pupils. St a t e a m e n d m e n t s a n d lo ca l r e gu la t io n s o r h o sp it a l p o licie s m a y d ict a t e t h a t m o r e t h a n 1 p r a ct i tioner must concur on the diagnosis. It is incumbent that the practitioner know the relevant regu lations earlier than m aking the diagnosis. Ce r e b r a l a n g io g r a p h y Re q u ir e s a b s e n ce o f ce r e b r a l b lo o d flo w, w h ich is in co m p a t ib le w it h b r a in s u r v iva l. Cons: expensive, time-consuming, requires trans port of the patient to x-ray department, invasive, doubtlessly damaging to organs which may be used for d on at ion, an d is n ot decide im al for d etect in g sm all am ou n t of blood blow t o mind stem. Criteria: absence of intracranial flow on the level of the carotid bifurcation 5 or circle of Willis). Not routinely used in the diagnosis of mind dying, but may be employed in di cult situations. Necessitates transport to the radiology/nuclear medication depart ment and requires an experienced interpreter. There m ay be delayed or faint visualization of dural venous sinuses even with mind 15 dying due to connections between the extracranial circulation and the venous system. Fa ls e p o s it iv e r a t e h a d n o t b e e n d e t e r m in e d in c o m a t o s e n o n b r a in d e a d p a t ie n t s. An 16 different criteria is disappearance of the P14 peak (substrate: medial lem niscus and nucleus cuneatus) on nasopharyngeal electrode recordings. Movements are sometimes complex in nature, and will occur as long as 32 hours after mind dying. Documented observations embody: facial actions, finger tremor, repeti tive leg actions, and even sitting up. Th is t yp ica lly o ccu r s w it h a ve n t ila t o r t h a t is s e t t o t r ig ge r o n d e t e ct ing respiratory e ort. Ventilators may be sensing air movement created by transmission of arterial pulses of the nice vessels to the lung or actions of a chest tube. Re co m m e n d e d o b s e r v a t io n p e r io d s b e t w e e n e x a m s: Fo r t e r m n e w b o r n s (three 7 w e ek s ge st a t io n a l a ge) t h r o u gh three 0 d ays o f a ge: 2 4 h o u r s Fo r in fa n t s a n d ch ild r e n (> three 0 d ays t o 1 8 ye a r s): 1 2 h o u r s Fo llow in g ca r d io p u lm o n a r y r e su scit a t io n, t h e d ia gn o sis o f b r a in d e a t h sh o u ld b e d e fe r r e d 24 hrs if there are concerns or inconsistencies in the examination ination 19. M a n y h o s p it a ls h a ve d e ve lo p e d �Ca t a s t r o p h ic Br a in In ju r y� order units to address these predictable penalties. Hyp o t e n sio n With hypovolemia due to diabetes insipidus and destruction of the pontine and medullary vasomo tor centers most mind lifeless sufferers are hypotensive. Treatment requires restoration of a euvolemic state and support with vasopressors. Usually norepinephrine to provide inotropic support and neo synephrine to improve peripheral vascular resistance is su cient to support the blood stress. Dia b e t e s in sip id u s With lack of hypothalamic operate mind lifeless individuals regularly have posterior pituitary dys operate and diabetes in sipidus. This is m anifest by giant volum e dilute urin ary output, hypernatre mia and hyperosmolar serum. The vasopressin drip may be preferable as a result of the shorter duration of action may help keep away from oliguria due to overdosing. Hyp o t h e rm ia Lo s s o f t e m p e r a t u r e r e g u l a t i o n fr e q u e n t l y c a u s e s h y p o t h e r m ia w h i c h c a n w o r s e n c o a g u l o p a t h y a n d invalidate mind dying testing. Application of a warm ing blanket to support temperature w sick help restore normal physiology. The timeframe from authorization until organ restoration regularly takes 24 to 36 hours or longer. Organs usually recovered in this manner: kidneys, liver, pancreas, lungs, 21 and infrequently the guts. Co n s e n t Prior to any discussion of donation, the fam ily should have m ade their determination to w ithdraw support and allow the patient to progress to dying. Consent must also be obtained for any donation-related procedures previous to dying (which typically consists of heparin infusion to prolong 24 organ viability and the possibility of femoral catheters). Cle a r a n ce fr o m t h e m e d ica l e x a m in e r m u s t b e o b t a in e d in a p p lica b le ca s e s (in clu d in g d e a t h s d u e to accident, homicide, suicide). Procedure Li fe s u s t a i n i n g m e a s u r e s a r e d i s c o n t i n u e d (t y p i c a l l y c o n s i s t i n g o f e x t u b a t i o n) u s u a l l y i n t h e o p e r a t ing room. After declaration of dying, cold perfusion of organs is per for m e d an d t h ey are p rocu purple. To a v o i d p o t e n t i a l c o n f l i c t s o f i n t e r e s t, n o m e m b e r o f t h e t r a n s p l a n t t e a m c a n p a r t i c i p a t e i n e n d 21 of-life care nor the declaration of dying. In these cases, organ donation is can celled, the household m ust be imm ediately notified, and end-of-life care continues. Scalp, earlobe and nasopharyngeal cal Problems in Medicine and Biomedical and recordings of the median nerve somatosensory Be h a vior a l Re se a rch. Systemic Atropine mind dying in adults: report of the Quality Stand Ad m in ist r a t io n Du r in g Ca r d ia c Ar re st Doe s Not ards Subcommittee of the American Academy of Ca u se Fixe d a n d Dila t e d Pu p ils. The Apnea dren: an update of the 1987 Task Force recommen Test for th e Determ in at ion of Brain Deat h. Spinal Man [23] Committee on Non-Heart-Beating Transplantation Aft e r De cla r at io n o f Br a in De a t h. Confirmation of Br a in De a t h w it h Po r t a b le Iso t o p e An gio gr a p h y: A 19 e-surg. Community acquired meningitis is a medical emer gency, and ought to be treated im m ediately.
Buy 10mg isordil. न्यूमोनिया का इलाज घर पर कैसे करें।Pneumonia disease treatment.
Slit -lam p e xam sh ow s som e p ar t s of ir is con t r act an d ot h e rs d on �t symptoms lung cancer proven isordil 10mg. Den er vation supersen sitivit y: usually happens after several w eeks (n ot in acute ph ase) medications may be administered in which of the following ways trusted isordil 10 mg. Miosis (constric tion) will occur in Adie�s pupil within half-hour (normal pupils will react only to medications vs medicine order 10 mg isordil 1%pilocarpine) treatment quinsy 10 mg isordil. Pharm acologic pupil Ge n e r a l in fo r m a t io n Fo llow s a d m in ist r a t io n o f a m yd r iat ic a ge n t. May current with accompanying H/A, and whether it is unknown that a mydriatic is involved, this may be misinterpreted. A p h a r m a co lo gica lly d ila t e d p u p il is ve r y la r ge (7 �8mm),and islarger than typicalmydriasisdue to third nerve compression (5�6mm). To d i erentiate pharmacologic pupil from a 3rd nerve lesion: instill 1%pilocarpine (a parasym pathomimetic) in each eyes (for comparison). Man age m e nt 32 Option: adm it an d obser ve overn igh t, pupil sh ould n orm alize. Usin g m ydr iat ic agen t s t o produ ce pu pillar y dilat ation In d icat ion s: t o im p rove t h e abilit y t o e xam in e t h e ret in a. This could mask pupillary dilatation from third nerve compression due to herniation. Always alert different caregivers and place a observe in the chart to document that the pupil has been pharmacologically dilated (see above), together with the agent(s) used and the time administered. Ocu lo m o t o r n e rve co m p ressio n Th ir d n e r ve co m p r e ss io n m ay m a n ife st in it ia lly w it h a m ild ly d ila t e d p u p il (5 �6mm). Possible etiol ogies include uncal herniation or enlargement of a p-comm or basilar bifurcation aneurysm. However, within 24 hours,most ofthese circumstances may also develop an oculomotor palsy (with down and out devi ation of the attention and ptosis). These pupils respond to mydriatics and to miotic brokers (the latter helps di erentiate this from a pharmacologic pupil, see above). Unilateral findings on the involved side in a fully developed Horner�s syndrome are proven in Ta b le 3 2. Thiswillbe accentuated by darkening the room, which causes the traditional pupil to dilate. Enophthalmos is because of Muller�s muscle paralysis, which also contributes a maximum of 2mm tothe ptosis. Possible sites of disrupt ion of sym pathetics Ge n e r a l in fo r m a t io n Se e also an a tom y of 1 st, 2 n d, an d 3 r d ord e r sym p at h et ic n e u r on s (p. Et io lo gie s o f d ysfu n ct io n: n e ck t r a u m a, ca r o t id va scu la r d ise a se / st u d ie s �. Ap r a clo n id in e o p h t h a lm ic (Io p id in e ) h a s e ss e n t ia lly r e p la ce d co ca in e fo r e st a b lis h in g d ia gn o s is. Iopidine causes the miotic pupil to dilate in Horner�s syndrome due to denervation hypersensitivity in the pupilodilator muscle fibers. Th e fr o n t a l e ye fie ld is t h e co r t ica l a r e a t h a t in it ia t es vo lu n t a r y (su p r a n u cle a r) la t e r a l s a cca d ic e ye movements (�pre-programmed�, rap id, ballist ic) t o t h e opposite side, involved in suppressing reflex ive saccades and producing voluntary, non-visible saccades. It is situated in Brodm ann�s area eight (in the fron tal lobe, an terior to th e prim ar y m otor cortex, Fig. The nerve passes through the cavernous sinus and enters the superior orbital fissure where it divides right into a superior division (innervating the superior rectus and the levator palpebrae superioris) and an inferior division (supplying the medial rectus, inferior rectus and inferior indirect). The parasympathetic fibers travel with the inferior division and branch e-surg. Postganglionic fibers enter the posterior globe to innervate the ciliary m uscle (relaxes the lens w hich �thickens� and accommodates for near vision) and the constrictor pupillae muscle. No n p u p il-sp a rin g o cu lo m o t o r p a lsy Th e r u le o f t h e p u p il in t h ir d n e r ve p a ls y Elu cid at e d in 1 9 5 eight b y Ru cke r. In e ect, states �Th ir d n e r ve p a ls y d u e t o extrinsic compression of the nerve might be related to impaired pupillary constriction. Develop m en t of a n ew 3rd n er ve p alsy ip silateral t o a p -com m an eu r ysm m ay be an indication of enlargement with the potential for imminent rupture, and is traditionally considered a sign for pressing treatm ent b) aneurysms of the distal basilar artery or bifurcation (basilar tip) c) carotid-cavernous fistula (p. Ot h er cau ses o f o cu lom o t o r p alsy Tr a u m a, u n c a l h e r n ia t i o n, l a t e r a l l y e x p a n d i n g p i t u i t a r y a d e n o m a s, Ly m e d i s e a s e, c a v e r n o u s s i n u s lesions: usually cause extra cranial nerve findings; see Multiple cranial nerve palsies (cranial neuropathies) (p. Le s i o n s w i t h i n t h e o r b i t t e n d t o a ect 3rd nerve branches unequally. Superior division lesion > ptosis and impaired elevation; inferior division lesion > im pairm ent of depression, adduction and pupillary response. Trochlear nerve axons pass dorsally around the aqueduct and decussate internally just caudal to the inferior colliculi. The nerve innervates the superior indirect muscle which primarily depresses the adducted eye, however in main gaze it intorts and secondarily abducts and depresses the globe. It m ay occasion ally occu r w it h lesion s of t h e cerebral peduncle or injury to the floor of the fourth ventricle near the aqueduct. Most circumstances resolve within 3 months (different cause must be sought in circumstances lasting longer) 2. Usu ally seen in diabetic or immunocompromised patients, sometimes in in any other case healthy 20 patients. Often involves dural sin uses an d m ay cause cavern ous sin us th rom bosis d) mets e) lymphoma 2. An idio pathic inflammatory disease confined to the orbit which will mimic a true neoplasm. Ra d ia t io n t r e a t m e n t w it h 1 zero zero zero �2000 rads may be needed for circumstances of reactive lymphocytic hyperplasia. The pupil is usually spared (frequently not the case with aneurysms, specific irritation, etc. Th e c a u s e i s o ft e n 22 not decided, however may not often be due to aneurysm compressing V1 w ith sympathetics. Elicit in g t h e co r n e a l r e fle x p r o d u ces a jaw je r k o r co n t r a la the r a l ja w movement (ipsilateral pterygoid contraction). Aprimitive pontine reflex,may be seen in quite a lot of insults to the brain (traum a, intracerebral hem orrhage). Rh yt h m ic, ir r e gu la r p u p illa r y o scillat io n s, ch a n gin g b y 2mm. Mayconfuse examination when checking pupillary responses; record the initial response. Opening the mouth causes opening ofa ptotic eye (irregular reflex between proprioception ofpterygoid muscular tissues 32 and third nerve). Seen only in patients with peripheral facial nerve accidents, and doubtless results from aber rant regeneration. Ab r u p t, s p o n t a n e o u s, co n ju ga t e d o w n w a r d e ye d e by way of t io n w it h s low r e t u r n t o midposition,2 to 12 occasions per min. It is related to bilateral paralysis ofhorizontalgaze,includ ing to doll�s-eyes and calorics. Most generally seen with destructive lesions of the pontine tegmen tum (usually hemorrhage, but also infarction, glioma, trauma), however has also been described with 24 compressive lesions. At yp ica l b o b b in g is sim ila r e xce p t t h a t h o r izo n t a l ga ze is p r e s e r ve d, a n d ca n be seen with cerebellar hemorrhage, hydrocephalus, trauma, metabolic encephalopathy 25 Opsoclon u s. Vis u a l s e n s a t io n t h a t s t a t io n a r y o b je ct s a r e s w a y in g s id e t o s id e o r v ib r a t in g. Ra r ely t h e so le m a n ife st a t io n o f Ch ia r i I m a lfo r m a t ion 27 (typically related to downbeat nystag 28 mus). Li d r e t r a c t i o n o n d o w n w a r d g a z e (t r u e v o n Gr a fe s ig n i s l i d l a g i n h y p e r thyroidism) seen in aberrant nerve regeneration (inferior rectus innervation > activation of levator palpebrae). Ch r o n ic, p r o g r e s s ive o p t ic a t r o p h y is d u e t o a co m p r e ss ive le s io n (a n e u r y s m, m e n ingiom a, osteopetrosis) until confirmed in any other case. Lithium-Induced Sparin g Oculom otor Nerve Palsy due to Midbrain Dow nbeat Nystagm us.
Plantain (Water Plantain). Isordil.
- Are there safety concerns?
- How does Water Plantain work?
- Bladder and urinary tract diseases.
- Dosing considerations for Water Plantain.
- What is Water Plantain?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96365