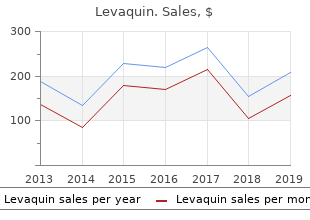
Levaquin
"Proven 500 mg levaquin, medicine 8 soundcloud".
By: L. Lester, M.B.A., M.D.
Associate Professor, University of North Texas Health Science Center Texas College of Osteopathic Medicine
The Internet and other electronic support could be a supply of knowledge and support for monitoring withdrawal symptoms cheap levaquin 750 mg, providing feedback and growing motivation treatment vertigo order 250 mg levaquin, aiming to treatment associates generic levaquin 250mg support self-administration and adherence medicine jar quality levaquin 500mg. Moreover, not all data associated to Parkinson�s shall be applicable to every pwp�s needs. Some pwp may choose easy sms reminders to perform workout routines, whereas others may choose utilizing a Parkinson exercise app ( Also available are exercise diaries or data from exercise displays that can be shared on-line. These give pwp insight into their daily physical exercise levels (did I obtain my personal targets In addition, on-line well being communities can be used to share experiences, exchange information, and improve illness-specifc experience, but in addition to bridge geographical distances and allow interdisciplinary coll aboration across establishments and conventional echelons. Despite this, in 2011, 42% of the folks aged 55 to 64 years and sixty five% of those aged sixty five to 74 years had by no means used the internet570. In general, these percentages are greater for japanese and 87 European Physiotherapy Guideline for Parkinson�s illness southern Europe, and decrease in northern and western Europe. It is essential to keep the circumstances of measurement stable, especially the situation and time of measurement (5. Doing so, it is very important keep in mind that pwp are, by the character of the illness, losing function454. For feasibility function, make the activities performed with the selected tools a part of your treatment plan. To consider pwp satisfaction with physiotherapy care offered, the MedRisk Instrument is out there (copyrighted and owned by MedRisk). Validated versions of this instrument are available in English, Spanish and Italian, and more are underway. When requirements for communication are available via the national physiotherapy affiliation, these ought to be followed. Finally, if required, the physiotherapist can help in referral towards palliative care. Moreover, Parkinson�s illness is progressive, thus along with current impairments and exercise limitations, new ones could be expected. Physiotherapists could be considered the physical drugs consultants in the administration of Parkinson�s illness. Pwp could be supported in their self-administration by the provision of tools such as the Exercise Diary (Appendix 5. Moreover, they are often guided towards group support groups and exercise courses. If for example a telephone or email is offered, agree upon who will originate the contact and when. Time to a next appointment for comply with-up or monitoring will depend on the pwp specifc circumstances and desires. Carers and, if applicable, home care professionals could be assisted in understanding motion associated issues in pwp (Appendix three). The treatment objective on this section is to preserve vital capabilities and to stop issues, such as strain sores and contractures. Exercise and motion technique training may still be effcacious, but scientifc analysis for this group of pwp is missing. Generally, the 5% to 10% of pwp staying in institutionalised, long term care amenities, receive suboptimal care by well being professionals without Parkinson�s-specifc expertise161. Furthermore, the experience of the occupational therapist is used in the number of strain relieving merchandise such as pillows, and the adjustment of wheelchairs and beds. In this chapter, results are offered per core area, consequence and sort of intervention (Table 7). Quality of life is one of the overall targets of Parkinson administration is to optimise high quality of life (2. Quality of life is infuenced by a wide range of impairments, exercise limitations, restrictions and private and environmental components. Given the scope of this Guideline, this data concentrates on physical exercise and motion activities. Others things to think about embody your medicine consumption, vitamin, speech, mood and sleep. Your neurologist or Parkinson�s illness nurse specialist will have the ability to inform you more about these, and refer you on to the suitable healthcare professional when wanted. Try to resolve on your own priorities and organise a balanced programme with the support of execs with Parkinson�s-specifc experience. Exercising regularly On average, folks with Parkinson�s illness are one-third less active than other folks of the same age. Not doing enough exercise can truly be more harmful to you than taking up exercise. Physical inactivity will increase the risk of developing antagonistic well being conditions, together with coronary heart illness, sort 2 diabetes and osteoporosis. If 30 minutes in one go is an excessive amount of, try shorter intervals, such as 3 times 10 minutes. For instance, try some exercise that helps you build muscle power in the future, then one thing that improves your endurance the subsequent day. Preferably choose practical-process workout routines, utilizing massive actions whilst mendacity down, sitting, standing or walking. This will improve your day-to-day perform, such as walking and and preserving your balance. For instance, some folks like enjoying a sport whilst others have to exercise while sitting or mendacity down. Please stop exercising and search medical advice should you break into a cold sweat or should you feel ache, nausea, tightness or ache in your chest for more than a few minutes, uncommon breathlessness, dizziness or mild-headedness or a sensation of your coronary heart skiping or adding beats. In all levels of the illness, a physiotherapist can give you advice and education. Physiotherapy treatment goals to stop, stabilise or scale back motion associated issues. You are suggested to seek the advice of a physiotherapist: � As soon as attainable after your prognosis for self-administration support. In some nations, referral by a physician or general physician may be necessary to get hold of reimbursement of your physiotherapy care costs. If you experience your major issues at your house, the physiotherapist may assess you at your house. If physiotherapy is indicated, you and the physiotherapist collectively set your particular person targets and develop a treatment plan. Physiotherapy treatment may embody a mix of advice, education, (home) exercise and training of so-referred to as compensatory strategies. The duration of a treatment period, in addition to the frequency of the visits will rely on your particular person targets and treatment plan. The physiotherapist will support you in your self-administration and subsequently focus on and agree with you upon time and means of ongoing contact. How typically you come to visit the physiotherapist will rely on your particular person circumstances and desires. Decide collectively what your targets of treatment ought to be: what to obtain, and by when This allows you to ask for feedback, for example to make sure you exercise appropriately. Remember that you have to keep active for so long as attainable, so agree upon the way to proceed at home upon completion of a treatment period. Agree upon what your physiotherapists should communicate to your referring physician. It provides you (and your carer) the chance to think about the issues you desire to the physiotherapist to tackle. This data will assist your physiotherapist in building a picture of what you think about your major issues, in addition to your physical capability. In the last 12 months, have you fallen at all for any cause, any journeys or slips, even if they in all probability had nothing to do with Parkinson�s illness Have you had any near misses in the last 12 months if you nearly did, but were in a position to stop a full fall
Interestingly symptoms sinus infection quality levaquin 500 mg, while perfusion of the lobster heart with every of the peptides usually ends in a lower in contraction frequency medicine - order 750 mg levaquin, every can elicit both a lower or an increase in contraction amplitude medications erectile dysfunction effective 250mg levaquin. No evidence of binding was noticed in non-transfected cells medications used to treat schizophrenia order levaquin 500 mg, indicating that binding is restricted to the expressed receptor. Differential receptor expression and activation by the three peptides may provide a proof for the differential responses of individuals to allatostatin-C. We are presently investigating evoked glutamatergic transmission as well as climbing fiber territory and plasticity. Synaptic Plasticity Support: Pinsent Darwin Scholarship Title: Neuronal pentraxin 2 binds to the perineuronal nets via hyaluronan 1 2 1 Authors: *H. We systematically characterized and categorized billions of individual synapses into 37 subtypes in mice based on synaptic molecular composition and bodily parameters, and generated the primary whole mind scale synaptome maps on the single synapse decision. Synaptome maps revealed exceptional complexity with many hitherto unknown anatomical options together with layers, patches and gradients of various subtypes of synapses. From single synapses on individual dendrites to the entire mind, striking and novel structure have been noticed in the spatial range of synapse subtypes. The hippocampus showed highest synaptic range with gradients that localize neural activity patterns and encode behavioral representations. Long-range connections and mesoscale connectome structure have been also outlined by synaptome maps. Mutations inflicting mental problems reprogramed international synaptome structure and reconfigured representations. We suggest that synaptome maps act as templates for the illustration of behaviors in the mind. The whole mind synaptome mapping resources reported here could be expanded to include different synapse proteins, outline new anatomical options and be built-in with different massive-scale mind map resources. Synaptome technology can be used in a wide range of basic science and medical studies. It can also be used along side connectomic and optogenetic strategies to tackle how the exceptional molecular and spatial range of synapses control the neural networks of the mind. Surprisingly, in imaging experiments, the GluN2B antagonist eliminated the vast majority of spontaneous events. Additionally, spines with prominent nanodomains showed a wider range of average peak amplitudes than spines that lacked nanodomains. When blocking glutamate transporters, lambda elevated to ~900 nm which also described the extracellular unfold of two-photon activated dyes in hippocampus. Using neuronally expressed iGluSnfr we verified that our estimates of lambda based on glutamate uncaging closely match the spatial action range of single action potential-driven glutamate launch from mossy fiber boutons. The useful influence of this synaptic cross-speak is even enhanced as a result of simultaneous spatially distributed glutamate uncaging events add in a supra-linear fashion at individual spines. Taken collectively, our knowledge problem the idea of level-to-level glutamatergic transmission and show that also the micron-scale spatial segregation of postsynaptic constructions is a relevant parameter for network computation and excitability. We explored these elements and the role of sodium diffusion using simultaneous sodium and calcium imaging (Miyazaki and Ross, 2015) from dendritic spines. We chosen dendrites near the floor where spines have been usually visible and positioned a stimulating electrode inside 20 �m of a dendrite. Single or paired shocks at 10 ms separation usually evoked localized (< 5 �m extent) fluorescence will increase similar to sodium and calcium concentration adjustments. The sodium signal rose sharply in the backbone and then appeared later in the close by dendrite. These responses are according to sturdy buffering of calcium and free diffusion of sodium. A pc model assuming elimination from the backbone only by diffusion reproduced the sodium alerts in the completely different compartments assuming backbone and dendrite dimensions from the literature and measured value for the sodium diffusion constant. In addition, the Mg block of the receptor is just relieved in the course of the short (~7 ms) epsp in the backbone, limiting the duration of sodium influx. Synaptic Transmission Support: Grants National Natural Science Foundation of China No. However, Parkin is extremely expressed throughout the mind and is a identified element of the postsynaptic density at glutamatergic neurons. Moreover, we find that the trafficking defects induced by Parkin loss-of-function result in impaired synaptic plasticity. In cytoplasmic compartments, the highest concentrations of synaptotagmin 1 are present in presynaptic terminals, nearly 40 % greater than in postsynaptic spines. However, these spines show about sixty five % greater concentrations than the corresponding dendritic shafts, and astrocytic processes showing only background levels of synaptotagmin 1. We further investigated whether postsynaptic synaptotagmin 1 is regulated during synaptic plasticity. In a rat model of chronic temporal lobe epilepsy, we discovered that pre and postsynaptic concentrations of the protein are reduced in comparison with control animals. This down regulation may be an adaptive measure to lower both pre and postsynaptic calcium sensitivity in excitotoxic circumstances. Components of the structure have been examined by Western blotting, immuno-dot blotting and immuno-gold negative staining electron microscopy. Shank3 accommodates a number of protein-protein interaction domains that hyperlink postsynaptic receptors to downstream signaling proteins and the actin cytoskeleton. They are important for constructing the structure of dendritic spines as their expression is enough to drive backbone formation and enlargement. Importantly Shank proteins are differentially expressed in mind areas critical for studying and cognition. In specific, Shank1 and Shank3 are both highly expressed in hippocampus and cortex. We discovered that Shank1/Shank3 deletion strongly scale back mice survival with a choose of mortality at P22-25. In summary, our outcomes reveal the important role of Shank1 and Shank3 in regulating hippocampal and cortical synapse maturation and function. Synaptic Transmission Title: Kalirin interacts with neuroligin relations as revealed by unbiased screens from mind and In situ analyses 1 2 1 1 Authors: *J. The Rho guanine nucleotide trade factor Kalirin has been implicated as an necessary mediator of many processes together with synaptic transmission and plasticity. The single Kalirin gene is alternatively spliced, leading to a number of isoforms; nevertheless, Kalirin-7 is the only mind specific protein variant. Kalirin has a number of binding companions which have been reported, though the mechanism by which Kalirin-7 regulates synaptic transmission, notably which protein-protein interactions are vital, stays largely unclear. To research Kalirin-7 protein interactions we first generated a Kalirin-7 specific antibody. Immunoprecipitating endogenous Kalirin-7 from mouse mind, we used liquid chromatography tandem mass spectrometry to display for potential Kalirin-7 interactors. These knowledge establish a novel isoform-specific interaction between two main proteins of the postsynaptic density. The massive extracellular domain of neuroligin-1 is responsible for transsynaptic binding with neurexin, a presynaptic cell adhesion molecule, and the short cytoplasmic tail of neuroligin-1 is exposed to a variety of intracellular regulation. The phospho-mimetic mutant also showed reduced floor expression levels in cultured neurons, which implies an impact of the phosphorylation in neuroligin-1 trafficking and further useful consequences in neurons. Wnt5a, a non-canonical Wnt ligand, is a morphogen appearing in the upkeep of dendritic arborization on hippocampal neurons. This results in suggest a key role of Wnt5a in the structure of excitatory synapses. On the opposite, it has been shown that Wnt5a protects neurons towards A forty two oligomers synaptotoxicity. Given the truth that Wnt5a seems to counteract the distresses caused by A forty two oligomers. These effects are exerted only by non canonical activation, via Wnt5a ligand and not by the canonical effects of Wnt7a. Removing the flr gene from specific mind areas would enable analyses of the pathways involved in the abnormal behaviors of Flailer mice. Ownership Interest (inventory, inventory choices, royalty, receipt of mental property rights/patent holder, excluding diversified mutual funds); Founder of Editas Medicine.
Buy 250 mg levaquin. Professor Olivares present Improvement in schizophrenia: Long and short term perspectives.
They are members of the viridans group of streptococci; hemolysis of blood agar is usually alpha or gamma symptoms 2 days before period buy levaquin 250mg. They require a nonshedding oral surface for colonization and are frequent residents of dental plaque treatment 7th feb cardiff safe levaquin 250mg. Early childhood caries occurs worldwide symptoms your dog is sick buy levaquin 750 mg, with highest prevalence in growing nations symptoms graves disease safe 500 mg levaquin. Disadvantaged children, no matter ethnicity or culture, and those with low birthweight, are most incessantly involved; enamel hypoplasia, which may occur because of compromised dietary status throughout formative levels of major dentition, is commonly related. Mother-to-youngster transmission occurs through switch of contaminated saliva by kissing the infant on the mouth or, more doubtless, by moistening the nipple or paci er or by tasting food on the infant�s spoon before serving it. Colonization by maternal organisms largely is determined by inoculum size; moms with intensive dental caries usually have high ranges of mutans streptococci in their saliva. To prevent dental caries of early childhood, promote good oral hygiene in moms and encourage early weaning from the bottle. Counsel mother and father and caretakers in regards to the dangers of dental caries from feeding children milk and other drinks containing sugar and of transferring saliva to a child�s mouth when moms and other caretakers have untreated carious tooth. Identi cation�An usually asymptomatic helminthic infection of the duodenum and upper jejunum. Clinical manifestations embrace transient dermatitis when larvae of the parasite penetrate the skin on initial infection; cough, rales and generally demonstrable pneumonitis when larvae pass through the lungs; or belly signs brought on by the grownup feminine worm within the intestinal mucosa. Symptoms of persistent infection could also be mild or extreme, depending on the intensity of infection. Classic signs embrace belly pain (usually epigastric, usually suggesting peptic ulcer), diarrhea and urticaria; generally additionally nausea, weight reduction, vomiting, weak spot and constipation. Intensely pruritic dermatitis (larva currents) radiating from the anus may occur; as can stationary wheals lasting 1�2 days in addition to a migrating serpiginous rash shifting several centimeters per hour across the trunk. Rarely, intestinal autoinfection with rising worm burden may lead to disseminated strongyloidiasis with losing, pulmonary involvement and demise, particu larly but not completely within the immunocompromised host. Diagnosis entails figuring out larvae in concentrated stool specimens (motile in freshly passed feces), within the agar plate methodology, in duodenal aspirates or, often, in sputum. Held at room temperature for 24 hours or more, feces may present growing levels of the parasite, together with rhabditiform (noninfective) larvae and lariform (infective) larvae (these have to be distinguished from larvae of hookworm species) and free-living adults. Serological tests based mostly on larval stage antigens are constructive in eighty%�85% of contaminated patients. Occurrence�Throughout tropical and temperate areas; more com mon in warm, wet regions. They penetrate capillary walls, enter the alveoli, ascend the trachea to the epiglottis and descend into the digestive tract to attain the upper part of the small intestine, the place development of the grownup feminine is accomplished. The grownup worm, a parthenogenetic feminine, lives embedded within the mucosal epithelium of the intestine, especially the duodenum, the place eggs are deposited. These hatch and liberate rhabditiform (noninfective) larvae that migrate into the intestinal lumen, exit in feces and develop after reaching the soil into both infective lariform larvae (which may infect the identical or a new host) or free-living female and male adults. The free-living fertilized females produce eggs that hatch and liberate rhabditiform larvae, which may turn out to be lariform larvae within 24�36 hours. In some individuals, rhabditiform larvae may develop to the infective stage before leaving the body and penetrate through the intestinal mucosa or perianal skin; the ensuing autoinfection may cause persistent infection for a few years. Incubation interval�From penetration of the skin by lariform larvae until rhabditiform larvae appear within the feces takes 2�4 weeks; the interval until signs appear is inde nite and variable. Period of communicability�As long as living worms stay within the intestine; up to 35 years in instances of autoinfection. Ivermectin is the drug of selection; thiabendazole or albendazole are much less ef cient alternatives. The major lesion (chancre) usually appears about three weeks after exposure as an indurated, painless ulcer with a serous exudate on the site of initial invasion. Invasion of the bloodstream precedes the initial lesion; a rm, non uctuant, painless satellite tv for pc lymph node (bubo) commonly follows. After 4�6 weeks, even with out speci c treatment, the chancre begins to involute and, in most cases, a generalized secondary eruption appears, usually accompanied by mild constitutional signs. A symmetrical maculopapular rash involving the palms and soles, with related lymphadenopathy, is traditional. Secondary manifestations resolve spontaneously within weeks to 12 months; all untreated instances will go on to latent infection for weeks to years, and one-third will exhibit tertiary syphilis indicators and signs. In the early years of latency, there could also be recurrence of infectious lesions of the skin and mucous membranes. In other instances, and unpredictably, 5�20 years after initial infection, disabling lesions occur within the aorta (cardiovascular syphilis) or gummas may occur within the skin, viscera, bone and/or mucosal surfaces. Death or serious incapacity hardly ever occurs throughout early levels; late manifes tations shorten life, impair health and restrict occupational ef ciency. The widespread use of antimicrobials has decreased the frequency of late manifestations. Fetal infection results in congenital syphilis and occurs with high frequency in untreated early infections of pregnant ladies. It incessantly causes abortion or stillbirth and will cause infant demise through preterm supply of low birthweight infants or from generalized systemic disease. For screening newborns, serum is preferred over twine blood, which produces more false-constructive reactions. Serological tests are usually nonreactive during the early major stage while the chancre remains to be present; a dark eld examination of all genital ulcerative lesions may be useful, notably in suspected early seronegative major syphilis. Occurrence�Widespread; in industrialized nations sexually ac tive young people between 20 and 29 are primarily involved. Syphilis is usually more prevalent in urban than rural areas, and in some cultures, in males greater than in females. Mode of transmission�Direct contact with infectious exudates from obvious or hid, moist, early lesions of skin and mucous membranes of contaminated people throughout sexual contact; exposure almost always occurs throughout oral, anal or vaginal intercourse. Transmission by kissing or fondling children with early congenital disease occurs hardly ever. Transplacental infection of the fetus occurs during the being pregnant of an contaminated lady. Transmission can occur through blood transfusion if the donor is within the early levels of disease. Infection through contact with contaminated articles could also be theoretically attainable but is extraordinarily uncommon. Health professionals have developed major lesions on the arms following unprotected medical examination of infectious lesions. Period of communicability�Communicability exists when moist mucocutaneous lesions of major and secondary syphilis are present. Lesions of secondary syphilis may recur with decreasing frequency up to 4 years after infection, but transmission of infection is uncommon after the rst yr. Transmission of syphilis from mom to fetus is most probable throughout early maternal syphilis but can occur throughout the latent interval. Infected infants may have moist mucocutaneous lesions which might be more widespread than in grownup syphilis and are a possible source of infection. Susceptibility�Susceptibility is common, although solely approxi mately 30% of exposures lead to infection. Congenital syphilis is prevented through serological examination in early being pregnant and again in late being pregnant and at supply in high prevalence populations; deal with those who are reactive. Teach methods of non-public prophylaxis relevant before, throughout and after exposure, especially the correct and consis tent use of condoms. Control of patient, contacts and the immediate environment: 1) Report to native health authority: Case report of early infec tious syphilis and congenital syphilis is required in most nations, Class 2 (see Reporting); laboratories must report reactive serology and constructive dark eld examinations in many areas. Patients ought to chorus from sexual intercourse until treatment is accomplished and lesions disappear; to avoid reinfection, they need to chorus from sexual activity with earlier partners until the latter have been examined and treated. All identi ed sexual contacts of con rmed instances of early syphilis uncovered within ninety days of examination ought to receive treatment. Serological testing is important to guarantee sufficient deal with ment; tests are repeated at three and 6 months after treatment and later as wanted. In a small proportion of patients treated for major or secondary syphilis, nontreponemal tests may stay constructive regardless of repeated treatment. Failure of nontreponemal tests to decline 4-fold by three months after treatment for major or secondary syphilis identi es those vulnerable to treatment failure. Careful evaluation of prior treatment and extra evalua tion could also be required. Penicillin-delicate pregnant ladies ought to have their al lergy con rmed with skin tests (main and minor penicillin determinants) if take a look at antigens can be found.
Gastrointestinal diseases: To tide the affected person over a crucial period of the illness in regional enteritis (systemic remedy) and ulcerative colitis medicine abbreviations generic 250mg levaquin. Hematologic issues: Acquired (autoimmune) hemolytic anemia medications given for uti buy levaquin 750mg, congenital (erythroid) hypoplastic anemia (Diamond-Blackfan anemia) medications to treat bipolar order levaquin 750 mg, idiopathic thrombocytopenic purpura in adults (intravenous administration only; intramuscular administration is contraindicated) medicine zoloft generic levaquin 500 mg, pure pink cell aplasia, selected instances of secondary thrombocytopenia. Miscellaneous: Trichinosis with neurologic or myocardial involvement, tuberculous meningitis with subarachnoid block or impending block when used concurrently with appropriate antituberculous chemotherapy. Nervous System: Acute exacerbations of multiple sclerosis; cerebral edema associated with main or metastatic mind tumor, or craniotomy. Ophthalmic diseases: Sympathetic ophthalmia, uveitis and ocular inflammatory situations unresponsive to topical corticosteroids. Renal diseases: To induce diuresis or remission of proteinuria in idiopathic nephrotic syndrome or that due to lupus erythematosus. Respiratory diseases: Berylliosis, fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate antituberculous chemotherapy, idiopathic eosinophilic pneumonias, symptomatic sarcoidosis. Rheumatic issues: As adjunctive remedy for brief-term administration (to tide the affected person over an acute episode or exacerbation) in acute gouty arthritis; acute rheumatic carditis; ankylosing spondylitis; psoriatic arthritis; rheumatoid arthritis, together with three juvenile rheumatoid arthritis (selected instances could require low-dose maintenance remedy). For the therapy of dermatomyositis, temporal arteritis, polymyositis, and systemic lupus erythematosus. Intramuscular corticosteroid preparations are contraindicated for idiopathic thrombocytopenic purpura. Injection into the deltoid muscle should be averted due to a excessive incidence of subcutaneous atrophy. Cardio-renal: Average and huge doses of corticosteriods can cause elevation of blood strain, salt and water retention, and increased excretion of potassium. These effects are much less likely to happen with the synthetic derivatives besides when utilized in massive doses. Literature stories recommend an apparent association between use of corticosteriods and left ventricular free wall rupture after a latest myocardial infarction; due to this fact, remedy with corticosteriods should be used with nice warning in these sufferers. Drug induced secondary adrenocortical insufficiency may be minimized by gradual reduction of dosage. With increasing doses of corticosteroids, the rate of occurrence of infectious complications increases. Do not use intra� articularly, intrabursally or for intratendinous administration for native impact in the presence of acute native infection. Special pathogens: Latent illness may be activated or there may be an exacerbation of intercurrent infections due to pathogens, together with those attributable to Amoeba, Candida, Cryptococus, Mycobacterium, Nocardia, Pneumocystis, Toxoplasma. It is really helpful that latent amebiasis or lively amebiasis be ruled out earlier than initiating corticosteroid remedy in any affected person who has hung out in the tropics or in any affected person with unexplained diarrhea. In such sufferers, corticosteroid induced immunosuppression could lead to Strongyloides hyperinfection and dissemination with widespread larval migration, often accompanied by extreme enterocolitis and doubtlessly fatal gram-negative septicemia. If corticosteroids are indicated in sufferers with latent tuberculosis or tuberculin reactivity, shut remark is necessary as reactivation of the illness could happen. During prolonged corticosteroid remedy, these sufferers should obtain chemoprophylaxis. Viral infections: Chicken pox and measles can have a extra severe or even fatal course in pediatric and adult sufferers on corticosteroids. Ophthalmic: Use of corticosteroids could produce posterior subcapsular cataracts, glaucoma with potential injury to the optic nerves, and will enhance the institution of secondary ocular infections due to bacteria, fungi, or viruses. Corticosteroids should be used cautiously in sufferers with ocular herpes simplex due to corneal perforation. Since complications of therapy with glucocorticoids are depending on the dimensions of the dose and the length of therapy, a risk/profit determination must be made in every individual case as to dose and length of therapy and as to whether day by day or intermittent remedy should be used. Cardio-renal: As sodium retention with resultant edema and potassium loss could happen in sufferers receiving corticosteroids, these brokers should be used with warning in sufferers with congestive heart failure, hypertension, or renal insufficiency. Endocrine: Drug-induced secondary adrenocortical insufficiency may be minimized by gradual reduction of dosage. Gastrointestinal: Steroids should be used with warning in lively or latent peptic ulcers, diverticulitis, fresh intestinal anastomoses, and nonspecific ulcerative colitis, since they may improve the danger of a perforation. Signs of peritoneal irritation following gastrointestinal perforation in sufferers receiving corticosteriods may be minimal or absent. There is an enhanced impact due to increased metabolism of corticosteriods in sufferers with cirrhosis. Special consideration should be given to sufferers 7 at increased risk of osteoporosis. Clinical improvement or restoration after stopping corticosteroids could require weeks to years. Psychic derangements could appear when corticosteroids are used, ranging from euphoria, insomnia, temper swings, personality adjustments, and extreme depression to frank psychotic manifestations. Drug Interactions: Aminoglutethimide: Aminoglutethimide could lead to a lack of corticosteroid-induced adrenal suppression. Amphotericin B injection and potassium-depleting brokers: When corticosteroids are administered concomitantly with potassium-depleting brokers. There have been instances reported during which concomitant use of amphotericin B and hydrocortisone 8 was adopted by cardiac enlargement and congestive heart failure. Antibiotics: Macrolide antibiotics have been reported to trigger a big lower in corticosteroid clearance (see Drug Interactions, Hepatic Enzyme Inhibitors). Anticholinesterases: Concomitant use of anticholinesterase brokers and corticosteroids could produce extreme weak point in sufferers with myasthenia gravis. Anticoagulants, oral: Coadministration of corticosteroids and warfarin often results in inhibition of response to warfarin, although there have been some conflicting stories. Therefore, coagulation indices should be monitored frequently to maintain the desired anticoagulant impact. Antidiabetics: Because corticosteroids could improve blood glucose concentrations, dosage adjustments of antidiabetic brokers may be required. Cyclosporine: Increased activity of each cyclosporine and corticosteroids could happen when the two are used concurrently. Ketoconazole: Ketoconazole has been reported to significantly lower the metabolism of sure corticosteroids by as much as 60%, leading to an increased risk of corticosteroid side effects. Aspirin should be used cautiously along side corticosteroids in hypoprothrombinemia. Vaccines: Patients on prolonged corticosteroid remedy could exhibit a diminished response to toxoids and stay or inactivated vaccines due to inhibition of antibody response. Corticosteroids can also potentiate the replication of some organisms contained in stay attenuated vaccines. Carcinogenesis, Mutagenesis, Impairment of Fertility: No adequate research have been performed in animals to determine whether corticosteroids have a possible for carcinogenesis or mutagenesis. Steroids could improve or lower motility and variety of spermatozoa in some sufferers. Corticosteroids have been shown to be teratogenic in many species when given in doses equal to the human dose. Animal research during which corticosteroids have been given to pregnant mice, rats, and rabbits have yielded an increased incidence of cleft palate in the offspring. Nursing Mothers: Systemically administered corticosteroids appear in human milk and could suppress development, interfere with endogenous corticosteroid manufacturing, or trigger other untoward effects. Because of the potential for severe antagonistic reactions in nursing infants from corticosteroids, a call should be made whether to proceed nursing, or discontinue the drug, bearing in mind the significance of the drug to the mom. Pediatric Use: the efficacy and safety of corticosteroids in the pediatric inhabitants are primarily based on the nicely-established course of impact of corticosteroids which is similar in pediatric and adult populations. Published research provide proof of efficacy and safety in pediatric sufferers for the therapy of nephrotic syndrome (>2 years of age), and aggressive lymphomas and leukemias (>1 month of age). Like adults, pediatric sufferers should be carefully observed with frequent measurements of blood strain, weight, peak, intraocular strain, and clinical evaluation for the presence of infection, psychosocial disturbances, thromboembolism, peptic ulcers, cataracts, and osteoporosis. The linear development of pediatric sufferers handled with corticosteroids should be monitored, and the potential development effects of prolonged therapy should be weighed in opposition to clinical benefits obtained and the provision of therapy alternatives. Other reported clinical experience has not recognized variations in responses between the elderly and younger sufferers. In basic, dose selection for an elderly affected person should be cautious, often beginning on the low finish of the dosing vary, reflecting the larger frequency of decreased hepatic, renal, or cardiac perform, and of concomitant illness or other drug remedy. Dermatologic: Acne, allergic dermatitis, burning or tingling (particularly in the perineal space, after intravenous injection), cutaneous and subcutaneous atrophy, dry scaly skin, ecchymoses and petechiae, edema, erythema, hyperpigmentation, hypopigmentation, impaired wound therapeutic, increased sweating, rash, sterile abscess, striae, suppressed reactions to skin tests, skinny fragile skin, thinning scalp hair, urticaria. Fluid and electrolyte disturbances: Congestive heart failure in vulnerable sufferers, fluid retention, hypokalemic alkalosis, potassium loss, sodium retention.