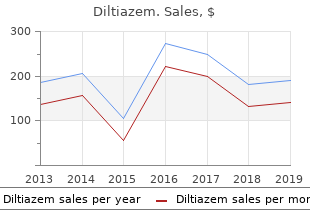
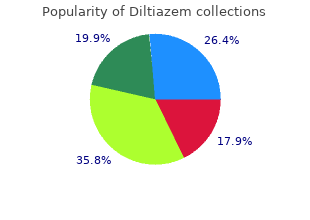
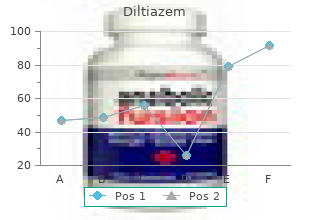
Diltiazem
"Safe 180mg diltiazem, medications j tube".
By: G. Lee, M.A.S., M.D.
Vice Chair, University of Cincinnati College of Medicine
It has been estimated that the majority youngsters develop no less than one episode of pharyn gitis per year 5 medications order 60mg diltiazem, 15–20% of which are caused by group A streptococci and nearly eighty% by viral pathogens (1 symptoms 37 weeks pregnant cheap diltiazem 60 mg, 5 treatment 5th finger fracture best 60mg diltiazem, 7 medicine plies safe 60mg diltiazem, 9). The incidence of pharyngeal beta-haemolytic streptococcal infections can vary be tween countries and inside the same nation, relying upon season, age group, socioeconomic situations, environmental factors and the quality of health care (1–three, 5, 10, 11). Surveys of healthy schoolchil dren 6–10 years of age, for example, found anti-streptolysin-O titres >200 Todd items in 15–70% of the children (2), while different research three reported beta-haemolytic streptococci service charges of 10–50% for asymptomatic schoolchildren (1, 2). In temperate countries, 50–60% of streptococci isolated from asymptomatic youngsters belong to sero logical group A, while streptococci in serological groups C and G together occur in less than 30% of the children. Conversely, in lots of tropical countries, groups C and G streptococci occur with charges as high as 60–70% in asymptomatic carriers (1–three, 5, 11). In either state, the affected person harbours the organism, but solely within the case of a real infection does the affected person show a rising antibody response. Therefore, many professionals really feel that solely sufferers with true infections have to be given antibiotics. Under endemic situations, group A streptococci have been isolated from sufferers with symptomatic pharyngitis. Group A streptococci are highly transmissible and spread rapidly in families and communi ties, with the predominant M sorts constantly changing. M serotypes 1, three, 5, 6, 18, 19, 24) have been obtained from the throat cultures of children within the affected commu nities (2, three, 5, 7, 19–23). Although no longitudinal research have examined tendencies in group A streptococcal pharyngitis, nor within the asymptomatic service charges, avail in a position data recommend that pharyngitis and asymptomatic service charges have remained extra-or-less steady in most countries (three, 5). However, within the last 20 years, some countries have reported modifications within the M sorts, severity and different characteristics of group A streptococci. More-virulent strains have re-emerged, for example, and non-M type streptococci have been detected (1–three, 5, 7, 11, 22). In the mid-1980s, the virulence, severity and sequelae of these infections also seem to have modified remark ably. A few research conducted in developing countries report incidence charges ranging from 1. The surveys outcomes showed there was extensive varia tion between countries, ranging from zero. Factors corresponding to a scarcity of sources for offering high quality health care, inadequate experience of health-care providers, 7 Table 2. Inadequate secondary Higher charges of recurrent prophylaxis and/or attacks with extra frequent non-compliance with and severe coronary heart valve secondary prophylaxis. Recent epidemiology of Group A streptococcal infections in North America and abroad: an outline. Epidemiology and prevention of group A streptococcal infection: acute respiratory tract infections, skin infections, and their sequelae at the shut of the twentieth century. Epidemiological evaluation of non-M-typeable group A Streptococcus isolates from a Thai inhabitants in Northern Thailand. Group A streptococcal sore throat in a periurban inhabitants of Northern India: a one-year prospective research. Asymptomatic pharyngeal carriage of beta-haemolytic streptococci and streptococcal pharyngitis among sufferers at an city hospital in Croatia. Effectiveness of scientific pointers for the presumptive treatment of streptococcal pharyngitis in Egyptian youngsters. Towards a better prognosis of throat infections (with group A beta haemolytic streptococcus) generally practice. The dynamics of streptococcal infections in a defined inhabitants of children: serotypes related to skin and respiratory infections. Group A streptococcal serotypes isolated from sufferers and siblings contact in the course of the resurgence of rheumatic fever within the United States within the mid-80s. Persistence of acute rheumatic fever within the intermountain space of the United States. The re-emergence of great group A streptococcal infections and acute rheumatic fever. Prevalence of coronary heart disease in school youngsters in rural Kenya utilizing colour-flow echocardiograph. Rheumatic coronary heart disease in a sub-Saharan African city: epidemiology, prophylaxis and health education. Fiebre reumática en Cuba: incidencia, prevalencia, mortalidad y caracteristicas clinicas. Rheumatic fever and continual rheumatic coronary heart disease in schoolchildren in Saudi Arabia. Epidemiological survey of rheumatic coronary heart disease among school youngsters within the Shimla Hills of northern India: prevalence and risk factors. Rheumatic coronary heart disease: prevalence and preventive measures within the Indian subcontinent. Prevalence of rheumatic fever and rheumatic coronary heart disease in school youngsters of Kathmandu city. A research of rheumatic coronary heart disease and rheumatic fever in a defined inhabitants in Sri Lanka. Rheumatic fever and rheumatic coronary heart disease within the Hamilton health district: an epidemiological survey. Acute rheumatic fever and rheumatic coronary heart disease within the prime end of Australia’s Northern Territory. Ten-year instructional programme aimed toward rheumatic fever in two French Caribbean islands. Rheumatic fever and continual rheumatic coronary heart disease in Yarrabah aboriginal group, North Queensland. The natural historical past of acute rheumatic fever in Kuwait: a prospective six-year observe-up report. There is consider in a position geographical variation within the prevalence of all serogroups of b-haemolytic streptococci. In many tropical countries, as much as 60–70% of isolates from the throats of asymptomatic youngsters fall into serogroups C and G. Conversely, in temperate areas, serogroup A is the predominant isolate (50–60%), with serogroups C and G to gether accounting for less than 30% of isolates. Post-streptococcal glomerulo nephritis might occur after an infection of either the throat or skin by nephritogenic strains of group A streptococci (1, 2). Major histocompatibiltiy antigens, poten tial tissue-specific antigens, and antibodies developed during and immediately after a streptococcal infection are being investigated as potential risk factors within the pathogenesis of the disease. Recent evidence means that T-cell lymphocytes play an important position within the pathogenesis of rheumatic carditis. It has also been postulated that particular M kinds of group A streptococci have rheumato genic potential. Such serotypes are normally heavily encapsulated, and form large, mucoid colonies which are wealthy in M-protein. These charac teristics enhance the ability of the micro organism to adhere to tissue, as well as their capability to resist phagocytosis within the human host. The streptococcal M-protein extends from the floor of the streptococcal cell as an alpha–helical coiled coil dimer, and shares structural homology with cardiac myosin and different alpha-helical coiled coil molecules, corresponding to tropomyosin, keratin and laminin. It has been instructed that this homology is answerable for the pathological findings in acute rheumatic carditis. Laminin, for example, is an additional cellular matrix protein secreted by endothelial cells that line the guts valves and is an integral a part of the valve construction. It can be a goal for a polyreactive antibody that recognizes M-protein, myosin and laminin. The M-protein molecule has a hypervariable N-terminal region, a conserved C-terminal region, and is split into A, B and C repeat areas on the idea of peptide sequence periodicity (5–7). Epitopes which are cross-reactive in myocardium, synovia and brain are located between the B and C repeat areas, away from the kind-specific epitopes within the N-terminal region. Individuals might have multiple streptococcal infections all through their lifetime, but reinfections with the same serological M type are relatively less widespread as a result of people acquire circulating homologous anti-M antibodies following an infection.
The diaphragmatic attachments have been divided medicine 512 cheap 180mg diltiazem, and the liver is retracted upwards and to symptoms tuberculosis proven 180 mg diltiazem the affected person’s left hair treatment cheap 60mg diltiazem. A giant retrohepatic vena caval department is ready for ligation and division (arrow) medicine 2410 best diltiazem 60mg. An different strategy has been described, which entails partial occlusion of the vena cava at the confluence of all three hepatic veins. This transhepatic strategy allows the transection of the remaining caudate parenchyma underneath direct vision of the middle hepatic vein, thereby minimizing the danger of damage. Total vascular isolation for caudate resection has additionally been described, however is normally pointless. In the latter case, tumor usually extends into the principal caudate duct, arising from the left hepatic duct, and caudate resection is necessary to achieve tumor clearance. The hilar plate must be lowered and Surgical administration of hepatobiliary and pancreatic issues fifty six the left side of the caudate Figure three. A clamp is passed between the inferior vena cava and the fibrous ligament (arrow), which in this case contains no hepatic parenchyma. The left portal vein and hepatic artery are exposed inside the porta hepatis and divided at some extent proximal to the principal caudate branches. Similarly, portal venous and hepatic arterial branches arising from the right must be sought and controlled. Once adequately exposed, the widespread trunk may be divided with a vascular stapler or oversewn. The liver tissue is then divided along the principal resection aircraft, encompassing the middle hepatic vein. The left hepatic vein may be divided during the hilar dissection or during parenchymal transection. It is crucial to avoid narrowing the biliary confluence when the left hepatic duct stump is oversewn. In this circumstance, the whole supraduodenal bile duct and lymphatic tissues are reflected upwards early within the process and included with the specimen. Also, the right hepatic duct must be divided at some extent past the tumor and earlier than dividing the liver. It may be essential to divide the duct at the level of the right anterior and posterior sectoral hepatic ducts. The bile duct margins must be sent for frozen part histology to ensure full tumor clearance. Adding caudate lobectomy requires exposing and mobilizing the caudate, as described above for left hepatectomy. With the left liver and caudate utterly prepared, the road of parenchymal transection is oblique from the right, anterior to the right hepatic vein and then carried posteriorly along the right border of the caudate. The tumor prolonged very close to to the insertion of the middle and right hepatic veins. Complete removing required an prolonged right hepatectomy and caudate lobectomy en bloc. Caudate resection with right hepatectomy Caudate resection is somewhat easier to perform in conjunction with right hepatectomy, primarily as a result of the doubtless hazardous disconnection of the right portion of the caudate is averted. The right hepatic artery and right portal vein are exposed inside the porta hepatis. Caudate lobectomy fifty nine can be utilized to retract the widespread bile duct and hepatic artery upwards and to the left, permitting entry to the portal vein from the right aspect 6 (Fig. A small posterolateral department to the right portion of the caudate is normally encountered (Fig. This department must be divided early within the dissection to avoid inadvertent damage and to enable higher exposure of the right portal vein. With the influx to the right lobe controlled, a clear line of demarcation must be evident along the principal resection aircraft. Dissection of the left portal vein at the base of the umbilical fissure exposes the. The liver is now fully mobilized off the vena cava by dividing the accessory hepatic veins. The right lobe have to be liberated from all of its diaphragmatic and retroperitoneal attachments. The falciform ligament must be divided to the extent of the suprahepatic vena cava, and the origin of the right hepatic vein identified. With the liver retracted upwards and to the left, ligation of the retrohepatic veins ought to begin from below and proceed to the extent of the hepatic vein 2, 6 (Fig. It is usually attainable to extend this dissection across the anterior surface of the vena cava and control some or all of the caudate veins. A clamp has been passed around the widespread trunk of the middle and left hepatic veins (white arrow). The left liver is now retracted upwards and to the right, and mobilization of the caudate Surgical administration of hepatobiliary and pancreatic issues 60 lobe is accomplished. The hepatic parenchyma may be divided simply to the right of the middle hepatic vein. When necessary, the middle hepatic vein may be divided, either extrahepatically or from inside the liver parenchyma. It is safer and easier to control the right duct by dividing and oversewing the primary right portal pedicle, which is encountered early during parenchymal transection (Fig. When this process is performed for hilar cholangiocarcinoma, the bile duct have to be approached as discussed above. Alternatively, these pedicles may be isolated and divided during the parenchymal transection phase. The main right pedicle is exposed (white arrow) and is ready for ligation and division. Since 1990, Caudate lobectomy 61 however, many centers have reported their experience with an increasingly larger number of procedures (Table three. In one of the largest collection of partial hepatectomy for hepatocellular carcinoma, caudate lobectomy was performed in less than 1% of sufferers. While some authors have reported a larger incidence of problems associated with caudate resection, four most collection cite morbidity and mortality figures that are comparable to these of standard hepatic resection. Some authors have advised that isolated caudate resection for metastatic tumors or hepatocellular carcinoma might not present adequate tumor clearance. Two research have documented narrow resection margins and early recurrences in sufferers present process isolated caudate resection for hepatocellular carcinoma and metastatic tumors. The numbers in parentheses point out the frequency of caudate resection as a percentage of all hepatic resections Author Number Diagnoses Procedures sixteen forty five Cholangiocarcinoma (forty five) En bloc full caudate Nimura et al. Moreover, research containing a larger number of full resections additionally report adequate tumor clearance and acceptable recurrence charges. The cumulated proof supports the efficacy of isolated full caudate lobectomy for small or medium sized tumors. Certainly, giant tumors normally require a extra in depth resection so as to achieve clear margins, and wedge resections, apart from very small tumors, must be averted. The results of several giant collection of resections for hilar cholangiocarcinoma, together with a report from the authors, help this coverage of selective caudate resection. While some lesions may be excised with an isolated caudate lobectomy, the majority will require right or left hepatectomy and caudate resection en bloc. In properly chosen sufferers, isolated caudate resection can achieve adequate tumor clearance without extreme morbidity. The surgical strategy to caudate resection is critically dependent on the size and site of the Caudate lobectomy 63 tumor. The surgeon must be utterly comfy with the related anatomy and the widespread variations, as well as the standard methods of hepatic resection. Complete resection of the caudate lobe of the liver: technique and results [review]. One hundred consecutive hepatic resections: blood loss, transfusion, and operative technique.
In addition medicine 852 proven diltiazem 60 mg, they each strongly agree that to treatment 8 cm ovarian cyst proven diltiazem 180mg sion symptoms 1 week before period cheap diltiazem 60 mg, somnolence and sedation in comparison with medications of the same type are known as cheap 180 mg diltiazem systemic opioids. They each strongly agree that when Anesthesiology 2014; a hundred and twenty:00-00 6 Practice Guidelines Copyright © by the American Society of Anesthesiologists. Food and Drug Administration posted a Box Warning to be added to the drug labels of codeine-containing merchandise in regards to the threat of codeine in postoperative ache management in kids after Recommendations for Criteria for Discharge to tonsillectomy and/or adenoidectomy. Preoperative initiation of continuous positive airway pressure frequent arousals throughout sleep. Anesthesiology 2014; a hundred and twenty:00-00 eight Practice Guidelines Copyright © by the American Society of Anesthesiologists. Extended keep in postanesthesia care unit versus no Limit procedures to facilities with full hospital companies prolonged keep in postanesthesia care unit. Hospital admission versus discharge home Intraoperative Management For the literature evaluation, doubtlessly relevant medical studies Anesthesia method had been identifed via digital and handbook searches of the lit-. More than 2,000 citations had been anesthesia initially identifed, yielding a complete of 835 nonoverlapping. Sedation versus common anesthesia articles that addressed subjects related to the evidence link Monitoring ages. Continuously monitor the respiratory depressant efects of sed direct evidence and had been subsequently eradicated. A air flow, oxygenation, and automatic apnea monitoring) complete bibliography used to develop these Guidelines. Special intraoperative monitoring methods (arterial organized by section, is out there as Supplemental Digital line, pulmonary artery catheter) Content 2, hyperlinks. Oral analgesics versus parenteral opioids rater chance-corrected settlement values had been (1) study. An updated opinion survey of place marketing consultant and American Society of Anesthesiologists mem-. Telemetry monitoring techniques versus no telemetry suspected obstructive sleep apnea was performed. The survey monitoring techniques price of return for the consultants was fifty three% (N = fifty four of 102). Monitored settings versus routine hospital wards and 267 responses had been obtained from the random sample of American Society of Anesthesiologists members. Anesthesiology 2014; a hundred and twenty:00-00 10 Practice Guidelines Copyright © by the American Society of Anesthesiologists. Pediatric patients: ° Intermittent vocalization throughout sleep ° Parental report of restless sleep, diffculty breathing, or struggling respiratory efforts throughout sleep ° Child with evening terrors ° Child sleeps in uncommon positions ° Child with new onset enuresis 3. If a sleep study has been done, the results must be used to determine the perioperative anesthetic management of a affected person. Anesthesiology 2014; a hundred and twenty:00-00 11 Practice Guidelines Copyright © by the American Society of Anesthesiologists. Invasiveness of surgical procedure and anesthesia Point rating: (0–3) Type of surgical procedure and anesthesia Points Superfcial surgical procedure beneath native or peripheral nerve block anesthesia without sedation 0 Superfcial surgical procedure with moderate sedation 1 or common anesthesia Peripheral surgical procedure with spinal or epidural anesthesia (with not more than moderate sedation) 1 Peripheral surgical procedure with common anesthesia 2 Airway surgical procedure with moderate sedation 2 Major surgical procedure, common anesthesia 3 Airway surgical procedure, common anesthesia 3 C. Requirement for postoperative opioids Point rating: (0–3) Opioid requirement Points None 0 Low-dose oral opioids 1 High-dose oral opioids, parenteral or 3 neuraxial opioids D. This example, which has not been clinically validated, is supposed solely as a guide, and medical judgment must be used to assess the risk of a person affected person. Consultant Survey Responses Percent Responding to Each Item Strongly Strongly N Agree Agree Equivocal Disagree Disagree I. Continued Percent Responding to Each Item Strongly Strongly N Agree Agree Equivocal Disagree Disagree 5. Continued Percent Responding to Each Item Strongly Strongly N Agree Agree Equivocal Disagree Disagree 22. Continued Percent Responding to Each Item Strongly Strongly N Agree Agree Equivocal Disagree Disagree 3. Continued Percent Responding to Each Item Strongly Strongly N Agree Agree Equivocal Disagree Disagree V. Anesthesiology 2014; a hundred and twenty:00-00 16 Practice Guidelines Copyright © by the American Society of Anesthesiologists. Clin Otolaryngol Allied Sci 2002; 27:344–6 Supported by the American Society of Anesthesiologists and 15. Address correspondence to the American Society of Anes 2013; [Epub ahead of print] thesiologists: 520 N. American Society of Anesthesiologists: Practice Guidelines for 19:410–eight the Perioperative Management of Patients with Obstructive Sleep Apnea. Lavie P, Herer P, Hoffstein V: Obstructive sleep apnoea syn drome as a threat factor for hypertension: Population study. Anesth Analg 2012; tinuous positive airway pressure therapy on 24-hour blood 115:106038–eight pressure in patients with obstructive sleep apnea syndrome. Seet E, Chung F: Management of sleep apnea in adults-func sleep apnea in patients with important hypertension. Ann tional algorithm for the perioperative period: Continuing Intern Med 1985; 103:190–5 professional growth. Diabetes Res Clin Pract 1991; thirteen:forty five–51 patients with and without obstructive sleep apnea beneath 24. Am J Respir Crit Care Med 1999; 159:1960–6 Investigating the relationship between stroke and obstruc 7. Kaw R, Pasupuleti V, Walker E, Ramaswamy A, Foldvary 1990; 336:261–4 Schafer N: Postoperative problems in patients with 27. Andersson L, Brattström V: Cephalometric analysis of per obstructive sleep apnea. Int J Oral Maxillofac Surg 1991; metric model for the obstructive sleep apnea syndrome. Rivlin J, Hoffstein V, Kalbfeisch J, McNicholas W, Zamel N, obstructive sleep apnea syndrome. Unal M, Oztürk L, Kanik A: the role of oxygen satura Relationship between cephalometric traits and tion measurement and body mass index in distinguishing obstructive websites in obstructive sleep apnea syndrome. Angle between non-apnoeic snorers and patients with obstructive Orthod 2002; 72:124–34 Anesthesiology 2014; a hundred and twenty:00-00 17 Practice Guidelines Copyright © by the American Society of Anesthesiologists. Biddle C: Comparative features of the airway throughout common Smirne S: Craniofacial cephalometric evaluation in habit anesthesia in obese sufferers of sleep apnea and matched ual snorers with and without obstructive sleep apnea. Pediatrics 1991; 88:132–9 tal discrimination in patients with upper airway resistance 56. Hochban W, Brandenburg U: Morphology of the viscerocra cussion seventy four–5 nium in obstructive sleep apnoea syndrome—Cephalometric 57. J Pediatr 1995; Obstructive sleep apneic patients have craniomandibular 127:88–94 abnormalities. Ann Relationship to polysomnographic measurement of respira Intern Med 1997; 127(eight Pt 1):581–7 tory disturbance. Lyberg T, Krogstad O, Djupesland G: Cephalometric analy naire: A device to screen patients for obstructive sleep apnea. Riley R, Guilleminault C, Herran J, Powell N: Cephalometric the identifcation of obstructive sleep apnea. J Nerv Ment Dis analyses and fow-volume loops in obstructive sleep apnea 2008; 196:429–31 patients. Eur Respir J screening instrument for obstructive sleep apnea in a dis 1999; thirteen:403–10 ease-specifc population. J Oral Maxillofac Surg 1995; fifty three:1150–4 metric model for the obstructive sleep apnea syndrome. Tangugsorn V, Skatvedt O, Krogstad O, Lyberg T: Obstructive Intern Med 1997; 127(eight Pt 1):581–7 sleep apnoea: A cephalometric study. Eur J Orthod 1995; Neck and whole body fats deposition in nonobese and obese 17:forty five–56 patients with sleep apnea in contrast with that in control sub 50. Am J Respir Crit Care Med 1998; 157:280–3 Obstructive sleep apnoea: A cephalometric study. Yu X, Fujimoto K, Urushibata K, Matsuzawa Y, Kubo K: Signifcance of the lateral pharyngeal partitions. Am J Respir Crit Cephalometric analysis in obese and nonobese patients Care Med 1995; 152(5 Pt 1):1673–89 with obstructive sleep apnea syndrome. Am J Respir Crit Care Med 2000; 162(2 Smirne S: Habitual snoring with and without obstructive Pt 1):740–eight Anesthesiology 2014; a hundred and twenty:00-00 18 Practice Guidelines Copyright © by the American Society of Anesthesiologists. Friedman M, Tanyeri H, La Rosa M, Landsberg R, sleep apnea protocol following surgical procedure and anesthesia.
The try and symptoms ruptured spleen effective diltiazem 60 mg find a really physiological crystalloid preparation for both scientific and medical work has been going on for over three quarters of a century and the results have inevitably been a compromise treatment coordinator quality 60mg diltiazem. In situations of peripheral circulatory failure or liver disease treatment trichomoniasis proven 180mg diltiazem, there may be increased endogenous lactate production or decreased capability to symptoms wisdom teeth trusted 180mg diltiazem metabolise infused lactate (Veech 1986). Clinicians ought to concentrate on the shortcomings of both options and take explicit care to tailor the dose of every to the pathophysiological condition being handled. This could depend upon the nutritional state and preliminary salt and water steadiness of the subjects studied. Although this phenomenon has not been studied particularly in normally nourished healthy volunteers with out extended fasting, previous work from our group has shown that in such people, whereas an excess water load (in the type of 5% dextrose) is excreted rapidly, an excess sodium chloride load is excreted very slowly, and causes persistent dilution of haematocrit and serum albumin (Chapter 10) (Lobo, Stanga et al. This research was undertaken to decide the effects on healthy volunteers of a 50 g oral glucose load on urinary excretion of sodium and water and modifications in serum biochemistry after an intravenous bolus of 2 L 0. Our speculation was that though glucose could affect the response to a sodium load under situations of nutritional depletion, extended hunger, harm and hypovolaemia, it may have little effect in healthy regular subjects who quick for less than 12 h. Volunteers with 208 continual sickness or acute sickness in the six-week period previous the research, those on regular treatment and people with a historical past of substance abuse had been excluded. Two venous cannulae had been inserted; one in every forearm and blood was sampled for full blood depend, haematocrit, serum electrolytes (sodium, potassium, chloride and bicarbonate), albumin, and osmolality, and blood glucose. The urine collected was analysed for osmolality and concentrations of sodium, potassium and glucose. Body weight and the aforementioned blood tests had been repeated at hourly intervals for six h. Postinfusion urine samples had been pooled and analysed for osmolality and concentrations of sodium and potassium. Data had been tested for statistical significance using Student’s t-paired check and the Wilcoxon signed ranks check. Subjects gained 2 kg in weight after every infusion and at the finish of 6 h, weight remained about 1 kg above baseline (Fig. The modifications in body weight corresponded with the quantity of urine excreted (Table 13. These findings are in contrast to earlier studies in which subjects had been preconditioned by both extended hunger or the stress of sickness and surgery (Bloom 1962; 212 Franch, Guirao et al. In studies designed to help survival of mariners in life rafts, he studied the effect of giving only 1200 ml of water per day and the effect of 50 and one hundred g oral glucose on water and sodium steadiness. The urinary sodium excretion in a subject over a 6 day quick was about 350 mmol, which corresponded with a loss of 2. This loss of sodium was reduced by somewhat over 50% by an oral consumption of glucose and it was discovered that maximal sparing was achieved by offering 50 g glucose per day. Gamble thought this discovering unexpected and had no explanation for it, though he was in a position to reveal that it was not as a result of the antiketogenic effect of glucose. He concluded that this phenomenon had a job in the maintenance of the extracellular fluid volume. The authors had been in a position to reveal significant weight gains in both teams over a two-week period. However, over the identical time period, patients receiving hypertonic glucose alone gained 0. This effect on salt and water steadiness of changing glucose with fats in parenteral vitamin preparations has additionally been demonstrated by Sitges-Serra’s group in both rabbit (Franch, Guirao et al. The authors counsel that the quantity of glucose is primarily liable for the modifications in salt and water steadiness. On the opposite hand, it has been shown, in diabetic patients, that acute hyperinsulinaemia can induce a reduced fractional sodium excretion, regardless of a relative resistance to the glucose reducing results of insulin (Gans, Bilo et al. In a research of the effects of insulin on sodium dealing with in regular subjects, Norgaard et al. This contrasts 215 with the suggestion that the effects of glucose on sodium metabolism are extended and the speculation that this may be influenced by delayed catecholamine exercise (Garcia-Domingo, Llado et al. In conclusion, due to this fact, the beforehand noticed effect of glucose, enhancing salt and water retention may be conditioned by prior hunger, nutritional or fluid depletion, or the response to harm. This effect may be mediated by way of insulin in view of the similar response seen following the initiation of insulin therapy in type I diabetes (Norgaard, Jensen et al. Bloom (Bloom 1962) in 1962 drew comparability between the diabetic affected person the place carbohydrate metabolism is limited by the deficit in carbohydrate utilization and the fasting affected person the place carbohydrate is unavailable. In both situations sodium excretion was decreased when carbohydrate utilisation was increased and was due to this fact dependant not on the level of serum glucose however on what was out there for metabolism. Clinically our findings counsel that under regular situations, glucose could not contribute to the sodium retention normally seen under these circumstances though in the presence of nutritional depletion and/or sodium deficiency, it may accomplish that, as shown by different works. Intravenous fluids are additionally the most typical hospital prescription, but the topic of fluid steadiness shares with that of vitamin a low degree of knowledge and commonplace of practice among junior docs due largely to an absence of coaching. Salt and water overload could typically be an inevitable consequence of resuscitation, but it may take up to three weeks to excrete this excess. It is essential due to this fact to avoid unnecessary overload by prescribing excessive maintenance fluids after the necessity for resuscitation has handed. Our audit of patients referred for nutritional assist showed that many had oedema and dilutional hypoalbuminaemia. The common weight excess, as a result of fluid overload, of those who had been via important care was 10 L. Nutritional assist with restricted volume and sodium content material, combined with diuretics, and in some instances concentrated salt-poor albumin, cleared the oedema over 7-10 days with a rise in serum albumin of 1 g/L for every kg loss in body weight as dilution was reversed (Chapter 3). These modifications had been accompanied by medical improvement and recovery of gastrointestinal perform. Following the observations of Mecray in 1937, of delayed gastric emptying associated with hypoalbuminaemia and saline excess, we randomised 20 patients, present process colonic surgery for most cancers, to obtain commonplace postoperative fluids (more than 3 L of water and 154 mmol sodium/day) or restricted fluids (less than 2 L water and 77 mmol sodium/day) (Chapter 6). The restricted group had zero fluid steadiness however the usual group gained 3 kg optimistic saline steadiness. Solid and liquid phase gastric emptying occasions (measured by twin isotope radionuclide scintigraphy) (Chapter 5) had been nearly regular in the restricted group however significantly longer in the usual group (median 72. In the usual group, passage of flatus was 1 day later (median 4 vs 3 days, P=0. We concluded that a small optimistic salt and water steadiness enough to cause 3 kg postoperative weight gain delays return of gastrointestinal perform and prolongs hospital keep in patients present process elective colonic resection. Our concerns over fluid steadiness management led us to survey practice and knowledge among 200 junior docs in the Trent Region (Chapter 7). Pre registration House Officers had been liable for prescribing in 89% of situations. Although respondents expressed confidence in their prescribing capability, less than 219 half had been aware of the sodium content material of 0. Our survey of advisor surgeons (Chapter eight) discovered that junior workers were given written guidelines in only 22% of situations. Only sixteen% felt that their juniors had been adequately skilled, 15% said that there was little coaching on the firm, 35% thought fluid steadiness charts inaccurate, and only 30% thought that postoperative patients had been receiving applicable fluid prescription. The literature is surprisingly sparse in regards to the response of regular subjects to crystalloid infusion. Studies had been due to this fact conducted in regular subjects to measure physiological responses to crystalloid options in frequent use. Serum albumin concentration fell in all subjects (20% after saline, sixteen% after dextrose), mainly as a result of dilution. While dextrose was rapidly excreted, two-thirds of the saline was retained after six hours, with continuing dilution of albumin and haematocrit. These observations illustrate the slowness with which salt and water is excreted, even in regular subjects, whereas water excess alone is rapidly and efficiently excreted. The research was repeated with 1 L infusions to outline hormonal responses (Chapter 11). Plasma renin and complete renin concentrations and angiotensinogen fell to a larger extent after saline than after dextrose (P<0. There was no significant difference between the response of plasma aldosterone, atrial natriuretic peptide and arginine vasopressin. In explicit, natriuretic peptide rose throughout both infusions, however fell to regular inside an hour, regardless of the optimistic sodium steadiness from the saline. This suggests that, 220 whereas fluctuations in water steadiness are handled efficiently via osmoreceptors and vasopressin, and saline deficiency is sensed by volume receptors and the renin angiotensin aldosterone system, the mechanism for dealing with sodium excess is passive and inefficient. Dilution of haematocrit and serum albumin was larger and extra sustained after saline than after Hartmann’s.
Effective 180 mg diltiazem. What causes anxiety in the body ? |Health NEWS.