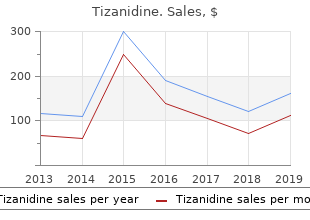
Tizanidine
"Proven tizanidine 2mg, muscle relaxant used during surgery".
By: S. Samuel, M.A., M.D., Ph.D.
Deputy Director, Center for Allied Health Nursing Education
It might require intensive interpretation of a number of databases and the appliance of superior know-how to muscle relaxant topical cream quality 2mg tizanidine handle the affected person spasms liver proven tizanidine 2 mg. Critical care may be provided on a number of days when the condition requires the level of doctor attention described above muscle relaxant antagonist generic 2mg tizanidine. However muscle relaxant toxicity order tizanidine 2mg, crucial care services may be provided in any location in uncommon circumstances. Reimbursement Reimbursement for crucial care codes is restricted to situations by which the doctor is offering fixed attention to the unstable critically ill affected person. Hospital care analysis and management codes should be used to report these services. Procedure code 99291 is billed to report as much as the first 30 seventy four minutes of crucial care service per day. This process code might solely be billed once per day by a person doctor or doctor of the same specialty inside a doctor group. Additional crucial care time increments should be billed using process code 99292 as shown in the chart below. Reimbursement for crucial care services exceeding 194 minutes or more than four items of 99292 on the same date of service requires submission of documentation with the claim that supports the medical necessity for prolonged crucial care and need for fixed doctor attention. Critical Care Time the next chart is used to appropriately bill for time spent performing crucial Reporting care services. For reporting by professionals, the next services are included in crucial care when carried out during the crucial interval by the doctor offering crucial care: � Interpretation of cardiac output measurements; � Interpretation of chest x-rays; � Pulse oximetry; � Blood gases and information saved in computer systems; � Gastric intubation; � Temporary transcutaneous pacing; � Ventilator management; and � Vascular entry procedures. Services Guidelines for In order to reliably and persistently decide that supply of crucial care Reporting Critical services rather than other analysis and management services is medically Care Codes needed, the next medical evaluation criteria should be met along with the definition of crucial care services: � Clinical Condition Criterion � There is a high likelihood of sudden, clinically important or life threatening deterioration in the affected person�s condition, which requires the highest level of doctor preparedness to intervene urgently; and � Treatment Criterion � Critical care services require direct personal management by the doctor. They are life and organ supporting interventions that require frequent personal assessment and treatment by the doctor. Withdrawal of or failure to provoke these interventions on an urgent basis would probably result in sudden, clinically important or life threatening deterioration in the affected person�s condition. Critical care services in a Teaching Facility teaching hospital might solely be billed using the time that the teaching doctor was in attendance and rendering service related to the individual affected person�s care. When a bill is submitted for a process code determined on the premise of time, the teaching doctor should be present for the time period for which the claim is made. December 2012 2-26 Practitioner Services Coverage and Limitations Handbook Critical Care Services, continued Critical Care in a Because crucial care is reported using time as the premise, the teaching Teaching Facility, doctor�s progress observe should comprise documentation of the whole time continued concerned offering crucial care services. When calculating time of a crucial care service in a teaching hospital, all of the following should be thought of: � Time spent teaching residents or medical students is probably not counted in the direction of the crucial care service time; � the teaching doctor should be present for the time period for which the claim is made; and � the teaching doctor should not bill time spent by the resident in the absence of the teaching doctor. Limitation on Place Critical care is expected in the hospital setting and is only reimbursable by of Service Medicaid when the critically ill or injured affected person is both admitted to the inpatient hospital or is anticipated as an admission to the inpatient hospital for continued crucial care. Non-Critical Care When a recipient continues to be positioned in the crucial care area of the ability, however is no longer critically ill, the supplier should bill subsequent hospital visits as a substitute of crucial care. Procedure Codes For pediatric and neonatal crucial care services, see the Pediatric Critical and Fees Care Services and Neonatal Critical Care Services sections in this chapter. December 2012 2-27 Practitioner Services Coverage and Limitations Handbook Custodial Care Facility Services Description Custodial care facility services are analysis and management services which might be provided to a recipient in a facility that gives room, board, and other personal help services, usually on an extended-term basis. Annual Medicaid reimburses for an annual comprehensive nursing facility assessment Comprehensive every one year. This process code is probably not billed along with the Nursing Facility month-to-month nursing facility analysis and management codes. Assessment Service Frequency Evaluation and management services for persistent care management are restricted to one medically-needed go to per thirty days, per supplier, per recipient. Acute Care Events Episodic care visits to handle acute occasions may be reimbursed if the attending practitioner is required to go to the affected person to make an alteration in the affected person�s treatment plan. The supplier should bill with a 22 modifier, and submit a report documenting the care provided. Services provided in an workplace or room positioned in a custodial care facility is probably not billed as workplace analysis and management visits. December 2012 2-28 Practitioner Services Coverage and Limitations Handbook Dialysis Services Description Dialysis services are these provided for the synthetic and mechanical removal of poisonous materials and the upkeep of fluid, electrolyte, and acid-base steadiness in instances of impaired or absent kidney perform. Service Medicaid reimburses for dialysis services rendered by or beneath the direct Requirements supervision of a doctor not salaried by the dialysis middle or hospital. Physician management and ongoing care of a dialysis recipient, exclusive of other medical conditions, are reimbursed as part of the dialysis service. Billing of Monthly or If a doctor supplies month-to-month or less than month-to-month, dialysis procedures for Less than Monthly the routine maintenance of a dialysis recipient, the medical document Dialysis Codes documentation should be maintained on the facility where the actual dialysis service is carried out. The doctor payments the month-to-month, or less than month-to-month, dialysis process codes using the place of service where he carried out the service of routine maintenance, not the place of service where the actual dialysis service was carried out. Inpatient Dialysis Medicaid will reimburse for dialysis services in the inpatient hospital setting in and Visits addition to one preliminary inpatient hospital consultation or one outpatient hospital consultation, as appropriate, and one discharge day management process code per recipient, per hospitalization. The hemodialysis procedures, including analysis and management services related to the recipient�s renal disease on the day of the hemodialysis process, may be reimbursed solely when provided in the inpatient hospital setting. These process codes are for the direct face-to-face supervision of a dialysis recipient. Services Included Services related to the recipient�s end stage renal disease which might be rendered on the day when the dialysis is carried out are included in the dialysis process. Evaluation and Management Services Description Evaluation and management services are face-to-face encounters with the recipient or the recipient�s family provided in the inpatient or outpatient hospital, recipient�s residence, or practitioner�s workplace. An exception to the face-to face encounter might occur when a doctor consultation happens through a telecommunications system in accordance with this handbook. Note: See Consultations, Custodial Care Facility Services, Nursing Facility Services, and Telecommunications in this chapter in this chapter for info on these kinds of visits New Patient Visit A new affected person is one who has not obtained any professional services from a practitioner throughout the past three years. December 2012 2-30 Practitioner Services Coverage and Limitations Handbook Evaluation and Management Services, continued Established Patient An established affected person is one who has obtained professional services from a Visit practitioner, or another practitioner of the same specialty who belongs to the same supplier group, throughout the past three years. On-Call On-call coverage and treatment of established patients for other practitioners should be billed with established affected person visits. Office Visits Office visits may be reimbursed for services provided in a practitioner�s workplace, an outpatient facility, or ambulatory facility. Home Visits Home visits may be reimbursed for a medically needed go to in the personal residence of the recipient. Hospital Visits Hospital visits to an inpatient recipient are reimbursable for under the next services: � Evaluation and management go to, and � Non-surgical service. Pediatric Primary Providers receive additional reimbursement for process codes 99212, Care Visits 99213 and 99214 provided to eligible recipients zero-19 years of age. December 2012 2-31 Practitioner Services Coverage and Limitations Handbook Evaluation and Management Services, continued Physician Standby Physician standby services are reimbursed for cesarean section standby solely. Visits A doctor standby service (process code 99360) is reimbursable along with the historical past and examination of the conventional new child toddler (code 99460) provided that: � Criteria for standby have been met (30 minutes or extra), and � Delivery was by cesarean section. Prolonged Services Prolonged practitioner service process codes will be reimbursed solely when all of the following criteria are met: � the practitioner has furnished and billed an analysis and management code; and � the time counted toward fee for extended analysis and management services contains solely direct face-to-face contact between the practitioner and the affected person whether or not the service was steady or not. The medical document should doc all of the following info: � the content material of the analysis and management service; and � the duration and content material of extended services that the practitioner personally furnished after the standard time of the analysis and management service is exceeded by at least 30 minutes. The time counted in the direction of using extended practitioner service codes is restricted to the sum of all direct practitioner-affected person face-to-face time beginning solely after the time required to carry out the content material of the billed analysis and management service is exceeded by at least 30 minutes. Visit After Hours When emergency services are provided in a supplier�s workplace at instances aside from frequently published workplace hours, Medicaid might reimburse for services requested after hours (process code 99050) along with the appropriate level of workplace go to. Hospital Observation services are these services furnished on a hospital�s premises, Observation including use of a mattress and periodic monitoring by a hospital�s nursing or other Services employees. They are services which might be reasonable and essential to consider an outpatient�s condition, or decide the need for a attainable admission to the hospital as an inpatient. Such services are coated when provided by the written order of a practitioner directing admission to statement services. December 2012 2-33 Practitioner Services Coverage and Limitations Handbook Evaluation and Management Services, continued Newborn Visit Medicaid reimburses for a historical past and examination of the conventional new child with Frequency in the the appropriate �V� analysis code once in the recipient�s lifetime. Hospital Medicaid reimburses as much as two subsequent hospital care visits for the analysis and management of a normal new child after the preliminary go to. Attendance at Medicaid reimburses for attendance of a doctor at supply (99464) for Delivery of preliminary stabilization of a new child (when requested by the delivering doctor) Newborn with the appropriate sickness analysis code. Infusion Therapy To be reimbursed for extended intravenous infusion, the presence of a Services doctor is required. Visit Office, residence, hospital, and emergency room visits are restricted to one go to, per Reimbursement recipient, per day, per specialty, aside from emergency services. Limitations Visits for general services (for example family practice) are restricted to two per thirty days for non-pregnant adults. Visits to the same recipient by a couple of specialty supplier on the same day are reimbursable.
The protracted hypomanic episode is the one such period we might document in this patient muscle relaxant kidney stones best tizanidine 2mg. It was not related to marked impairment at work spasms pelvic floor cheap tizanidine 2 mg, though the non-cease restless busyness he exhibited in bars distracted him from one girl to spasms film generic tizanidine 2mg one other spasms prozac best 2 mg tizanidine, with out reaching his sexual or romantic aims, leaving him extraordinarily frustrated and sad within the midst of his hypomania! Nonetheless, the cyclic course of the illness may contain periods of serious dysfunction, even serious suicidal makes an attempt (Dunner et al. By the same token the cyclic temper changes allow normal to tremendous-normal periods of perform ing (Akiskal et al. A not-inconsiderable number of these patients are capable of rebound from their tough periods, to attain new conjugal or occupational standing. Since her mid-teens she had experienced hypersomnic-retarded depressions lasting initially for a couple of weeks at a time and more recently for so long as 4 months; she estimated that she had had roughly one such episode per year, though she had skipped two years in a row twice. She had been hospitalized on two occasions; the primary time her family had been concerned about her not getting out of bed for days in a row, and the second time due to a severe postpartum episode during which she had been alternating between extreme fatigue and agitation and had verbalized thoughts of suicide. She was a profitable author, who wrote fiction, and had acquired considerable fame and wealth. Several occasions per year she experienced periods of decreased need for sleep, increased libido, intense joy, overconfidence, increased plans and activities each at work and in her private life. These hypomanic periods � which might final from a couple of days as much as per week � sometimes occurred at the tail finish of a despair, but at other occasions happened independently, after a night of sleep loss, typically "due to intense work". She said that men found her "too intense, too passionate", which has "wrecked my private life". She had been devoted to her first two husbands, however the separation from her third husband was precipitated by a short affair she had � with one other girl � during a hypomanic episode. She additionally felt extraordinarily heartbro ken as a result of she nonetheless beloved her final husband; moreover, in baby custody she had misplaced her 6-year-old daughter to her husband. After considerable discussion she was positioned on 1200 mg of lithium carbonate (blood level = zero. The patient complained of "lack of intensity", and after normal thyroid testing her regimen was modified to 600 mg of lithium (blood level = zero. She has been followed on this regimen basically euthymic with no opposed effects. Current analysis indicates that the more modal distribution for hypomania is 1�3 days (Akiskal et al. This is unfortunate as a result of patients with brief hypomania usually have a recurrent sample of periods of pleasure, that are followed by mini depressions, thereby fulfilling the criteria for cyclothymic disorder. This 24-year old, single female offered with historical past of "moodiness" since her menarche. The patient said at some point she would be "high like a kite" and the subsequent day she would stay in mattress. Her moods modified every few days, sometimes every day, but she was capable of end high school and worked as a receptionist in numerous jobs. At age 18 she began having more protracted "depressive" episodes twice a year, within the autumn and within the spring, lasting for 3�4 weeks. Upon closer scrutiny she indicated that the one within the autumn was characterized by sleeping too much and overeating, and the one within the spring by"a peculiar mixture of physical slowing, irritability, psychological restlessness and hypersexuality". She had obtained numerous the soft bipolar spectrumh 49 antidepressants for each types of "despair", to no avail. She was prescribed fluoxetine 20 mg/day, after 3 weeks she felt abruptly energized � her thoughts "running 200 miles a minute" � she might actually "climb the mountain" the place she lived, was overconfident, and slept with several men every day, the entire episode lasting 2 weeks. The patient had lived in six cities in three states since she was 18; she would simply take off unsatisfied with the place or the people. Over the previous year she was hospitalized as soon as for bulimic behaviour, and one other time for hurting herself with cigarette butts and hair curlers. Family historical past was vital in that the mom, considered "a flamboyant bitch", had been divorced 4 occasions, and had many lovers properly into her 70s; a maternal aunt, diagnosed manic-depressive, died in a psychological institution. Mental standing examination revealed a younger girl who complained that she was plump, with a particular flair in her attire � she truly appeared like a Hollywood star. Although her facial features displayed brilliant have an effect on, she said if lightning struck her lifeless, she would thank God. She spoke about her "utter failure to do anything right in life, despite being endowed with fairly good, native intelligence". She said her sister was like her, "solely worse, as a result of she uses every kind of substances, particularly uppers". Clinically, due to this fact, it might make quite a lot of sense to think about this patient as repeatedly shifting between cyclothymia and main despair. This formulation has vital therapeutic benefits, as a result of it might dictate the use of temper stabilizers nearly to the exclusion of antidepres sants. Failure to recognize bipolarity had robbed her of therapeutic alternatives that might have given her a more rewarding life. She subse quently made a dramatic recovery on lamotrigine monotherapy (slowly increased over 2 months to a dosage of 200 mg/day). At final comply with-up a year later she now not spoke of having been abused, but said "I am so like my mom that I should have imagined that her lovers did to her what I had fantasized as unacceptable sex. She additionally found secure gainful employment as an actress for the primary time in her life. It is noteworthy that, except for the primary two traits, lability is in a depressive path. This is a prevalent form of cyclothymia in each scientific and non-patient populations (Akiskal et al. We have more recently examined self-rated traits (Table 6) defining essentially the most discriminatory items for the cyclothymic disposition (Akiskal et al. This course of seems fairly different from clinically depressed patients who experience hypomania solely during antidepressant treatment. It may seem counter-intuitive that such patients ought to develop hypomania, but this has additionally been observed by others (Klein et al. What distinguishes these patients from the more garden-type variety of dysthymics is the fact that their family historical past is usually bipolar (Rosenthal et al. These patients can be considered phenotypic variants within the bipolar spectrum, repre senting much less penetrant forms of a putative bipolar genotype. This 47-year-old married girl gave a historical past of having been gloomy for so long as she remembered. Members of her family and colleagues would exhort her "to smile at life, so that life would smile at you". She said her stereotypical response would be breaking into tears; she was simply unable to smile. Despite these temperamental traits, the patient was a profitable college teacher, properly liked by college students and oldsters. The patient said she had little energy, but devoted most of it to her college students and their welfare. Despite a profitable profession of 25 years within the instructing area, she felt "grossly insufficient". Her sense of inadequacy was rein forced by her husband of about the same duration: He usually "abused her emotion ally", by which she meant he referred to as her "stupid" and complained of her "sexless nature". When their solely daughter left house at age 22, the patient made a suicide attempt with aspirin in a deepening despair with hopelessness, guilty rumina tions, poor concentration, and racing thoughts. She was treated (initially on an inpatient psychiatric unit), with a succession of full doses of no less than one antidepres sant from all existing lessons of antidepressants; her response was negative except for a transient 4-day sense of unusual properly-being and euphoria on tranylcypramine, forty mg/day. We found that her father had been treated for full-blown psychotic, manic-depressive illness; a paternal aunt had dedicated suicide, and a paternal uncle was a profitable politician who was identified to sleep very little. On psychological standing examination, the patient spoke with great rapidity and complained of maximum irritability. Over the subsequent 6 months the dosages of the 2 medications had been adjusted in such a method that she had drive and energy with out irritability, continued interest in her work and life, occasional "tears of happiness", while sustaining a point of reservation about how good life, marriage and men could possibly be. The couple obtained marital counselling which helped to rekindle a number of the misplaced romance in their marriage. It can be noteworthy that, while depressed, she exhibited no less than one hypomanic symptom racing thoughts or rapid speech. The family historical past helped in reclassifying this patient within the bipolar realm, and supplied the scientific rationale for the divalproex augmentation. The reason for creating this category is to deliver the attainable benefit of temper stabilization (Sonne and Brady 1999) to this group of patients who in any other case may be categorized as substance-induced or substance withdrawal-induced temper issues. This 29-year-old journalist had long indulged in cocaine and amphetamines in an try and make "my sturdy moods last longer".
Buy tizanidine 2 mg. Сколько мышц веса можно набрать за месяц использования киллограма Протеина Протеин для роста мышечно.
The inheritence pattern clothes muscle relaxant 24 tizanidine 2mg, too much make-up is most likely to spasms during period safe tizanidine 2mg be polygenic muscle relaxant medication prescription best tizanidine 2mg, however extra research is needed Behaviour Hyperactive muscle relaxant tmj best 2mg tizanidine, entertaining, irtatious, to establish the genes involved. The differential Pressure of thought prognosis of hypomania consists of mania, cyclothymia, I roll on like a ball, with this exception, that contrary to the hyperthyroidism, anorexia, and agitated despair. Hypo traditional legal guidelines of motion I even have no friction to deal with in mania could herald mania, and in such circumstances the prognosis my thoughts, and of course have some dif culty in stopping ought to be one of simply mania. Iam nearly sick and giddy with the amount of issues in my head � trains of thought beginning and branching to in nity, Cyclothymia crossing one another, and all tempting and eager to be Cyclothymia could be described as delicate chronic bipolar worked out. Flight of ideas Cyclothymia usually develops in early grownup life and is They thought I was within the pantry at house. Poor darling Catherine, you realize, Unless it progresses to bipolar affective disorder (15�50% 5 Catherine the Great, the re grate, I�m always up the of circumstances), it not often involves medical consideration. At work she took on many further hours and additional roles, however to her shock one of her colleagues reported her as unsafe. By then she couldn�t cease and behaviour are too persistent and marked to be included her ideas from racing and was sleeping only three or 4 hours a night. She turned very temper (for a minimum of several days on end), elevated energy outgoing and acted utterly out of character, dressing and activity, and usually marked feelings of properly-being and garishly, smoking marijuana, and getting herself arrested both physical and psychological ef ciency. Four months ago her temper talkativeness, overfamiliarity, elevated sexual energy, and a started dropping and she or he felt dreadful and ashamed. Today decreased need for sleep are sometimes present however to not the extent she is feeling higher however has had to promote her home to pay that they lead to extreme disruption of work or result in social off her debts. Irritability, conceit, and boorish behaviour could temper stabiliser, however she is understandably reluctant to take take the place of the extra traditional euphoric sociability. Self-esteem is in ated, and grandiose or over the next symptoms have continued (4 if the temper optimistic ideas are freely expressed. The particular person could embark on further 3 More talkative than traditional or stress to hold talking. D the disturbance in temper and the change in function are B During the period of temper disturbance, three (or extra) of observable by others. A the criteria are met both for a manic episode and for 6 Increase in aim-directed activity or psychomotor a major depressive episode (aside from duration) almost agitation. The Australian John Cade described the antimanic properties of lithium in 1949, however the drug took another 20 years to enter mainstream practice. It is subsequently import medicine, and uncover possible medical causes for the ant to examine renal function earlier than beginning the drug. Renal and thyroid function should Mood-stabilising and other medication also be monitored. Choice of medicine in bipolar affective disorder is Once started on lithium some sufferers cease taking it to a big extent determined by the patient�s current due to its facet-results (Table 5. It produces a faster Polyuria remedy and monitor every six months onset of action than both lithium or carbamazepine, and Polydipsia Hyperparathyroidism is of particular bene t in speedy cycling bipolar affective Stuffy nose, metallic Cardiotoxicity (T-wave attening on disorder. Valproate can cause neural tube defects and Nephrogenic diabetes insipidus other foetal malformations if used in being pregnant. These include nausea, headache, dizziness, of acute manic episodes, however takes several days to produce sedation, diplopia, ataxia, pores and skin rashes, rare however potentially an impact. If tolerated and effective, it ought to be continued deadly blood dyscrasias, and hepatotoxicity. Atypical antipsychotics may also be used within the acute the usage of anticonvulsants including valproate, carba remedy of mania and within the prophylaxis of bipolar mazepine, and lamotrigine within the prophylaxis of bipolar affective disorder, although speci c licensing agreements affective disorder is growing. All the generally used temper stabilisers (lithium, valproate, Drug Explanation and carbamazepine) are teratogenic and will ideally be Carbamazepine Can result in neurotoxicity; choose averted within the rst trimester of being pregnant. After a rst manic episode, about ninety% of sufferers experience further manic and depressive episodes, and the interepisode interval tends to turn into progressively Hospitalisation shorter. Hospitalisation is required in ultimately commit suicide, however the fee of attempted extreme circumstances if the patient can not function within the suicide is signi cantly higher. Virginia Woolf (1882�1941) I married, after which my brains went up like a bathe of within the Hours, a lm loosely based mostly on the novel Mrs Dalloway reworks. As an experience, insanity is terri c I can assure and starring Nicole Kidman as Virginia Woolf). This is her sui 5 you, and to not be sniffed at; and in its lava I still nd most cide note to her husband and carer: of the issues I write about. It shoots out of one every thing formed, nal, not in mere driblets as sanity does. So I am Quoted from a letter from Virginia Woolf to doing what seems the most effective thing to do. I don�t assume two individuals could have She felt very young; on the same time unspeakably aged. I can�t ght any sliced like a knife through every thing; on the same time was longer. You see I can�t even write had the feeling that it was very, very harmful to reside even this properly. You have been totally patient Virginia Woolf, Mrs Dalloway with me and extremely good. If anybody could have saved me it would have been Virginia Woolf, the novelist and member of the Bloomsbury you. Everything has gone from me however the certainty of your Group, suffered from bipolar affective disorder from the age of goodness. Summary Depressive issues Epidemiology Classi cation l the lifetime threat of depressive issues is about 15%. Aetiology l Genetic factors and environmental factors are both involved within the aetiology of depressive issues. All races and both endocrine situations, metabolic abnormalities, infections, sexes are equally affected. Aetiology Clinical features l Although genetic factors and environmental factors are l the scientific features of despair could be divided into core both involved within the aetiology of bipolar affective disorder, features, other common features, and somatic features. Clinical features Differential prognosis l the frequency and severity of episodes is very variable, as is l the differential prognosis of despair is from other psy the proportion of manic to depressive episodes. After a rst depressive episode, about 80% of sufferers have Management further depressive episodes. Churchill�s Black Dog and other Phenomena of the Human Mind 12 Interpersonal psychotherapy includes effecting change (1997) Anthony Storr. Renal and thyroid function must also be 5 One of the vulnerability factors for despair is loss monitored. Adverse outcomes are linked to household rejection, systemic discrimination and internalized homophobia. Barriers to remedy include prior negative experiences with clinicians concerning sexual identification, socioeconomic standing and marginalized standing. Epidemiology and Homosexuality � Estimates of the prevalence of men who establish of men who establish solely as homosexual, as homosexual differ from 1. The vary of reported prevalence identification prevents clinicians from understanding is determined by the way during which surveys are 3 3 social and personal facets of sexual identification. Most common causes systemic barriers and stigma which research show 2018 | psychiatry. These can include stress associated to disclosing relationships to 20 household, concerns for being safe in public areas, feeling judged as a same-intercourse couple and stress associated to unequal legal rights11. Gay Couples looking to 10 adopt a baby report elevated ranges of temper and nervousness issues in contexts with elevated systemic discrimination and decreased social 12. Where predominant social � Internalized homonegativity refers to the course norms stigmatize homosexuality, homosexual men encounter of negative social attitudes about homosexuality extra stigma and discrimination. These experiences 14 toward the self, leading to a devaluation of the self in flip lead to opposed psychological health outcomes. Negative public perceptions � Discrimination towards homosexual men can afect entry of homosexual men can lead to negative attitudes towards to work, medical health insurance and fnancial stability. Negative self value occurs extra often in Additionally, sufferers could fnd it harder to disclose single men18. Non-white men who establish as homosexual extra identification to healthcare suppliers and entry health often report feelings of internalized homophobia18 and social supports15. Experiencing discrimination 2 Barriers to accessing Mental Health Services � Gay men usually tend to report elevated � African American and Hispanic males report dissatisfaction and use of psychological health providers decreased entry and use of psychological health than heterosexuals19.
Hirabayashi K spasms under eye order 2mg tizanidine, Miyakawa J zyprexa spasms best 2 mg tizanidine, Satomi K spasms definition proven tizanidine 2mg, Maruyama T kidney spasms no pain quality tizanidine 2mg, Wakano K (1981) Operative results and postoperative progression of ossification amongst sufferers with ossification of cervical posterior longitudinal ligament. Hirabayashi K, Satomi K (1988) Operative procedure and results of expansive open-door laminoplasty. Hoshi K, Kurokawa T, Nakamura K, Hoshino Y, Saita K, Miyoshi K (1996) Expansive cervi cal laminoplasties � observations on comparative changes in spinous course of lengths fol lowing longitudinal laminal divisions utilizing autogenous bone or hydroxyapatite spacers. Kadanka Z, Bednarik J, Vohanka S, Vlach O, Stejskal L, Chaloupka R, Filipovicova D, Sure lova D, Adamova B, Novotny O, Nemec M, Smrcka V, Urbanek I (2000) Conservative treat ment versus surgical procedure in spondylotic cervical myelopathy: a prospective randomised examine. Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M, Hurri H, Koes B (2001) Multidisciplinary biopsychosocial rehabilitation for neck and shoulder ache amongst working age adults: a systematic review within the framework of the Cochrane Collabora tion Back Review Group. Kiray A, Arman C, Naderi S, Guvencer M, Korman E (2005) Surgical anatomy of the cervi cal sympathetic trunk. Kulkarni V, Rajshekhar V, Raghuram L (2004) Accelerated spondylotic changes adjoining to the fused section following central cervical corpectomy: magnetic resonance imaging examine evidence. Muro K, O�Shaughnessy B, Ganju A (2007) Infarction of the cervical spinal wire following multilevel transforaminal epidural steroid injection: case report and review of the litera ture. Nurick S (1972) the pathogenesis of the spinal wire disorder associated with cervical spondylosis. Ohshio I, Hatayama A, Kaneda K, Takahara M, Nagashima K (1993) Correlation between histopathologic options and magnetic resonance images of spinal wire lesions. Palit M, Schofferman J, Goldthwaite N, Reynolds J, Kerner M, Keaney D, Lawrence-Miya saki L (1999) Anterior discectomy and fusion for the management of neck ache. Panjabi M, White A, third (1988) Biomechanics of nonacute cervical spinal wire trauma. Peolsson A, Vavruch L, Hedlund R (2007) Long-term randomised comparability between a carbon fibre cage and the Cloward procedure within the cervical spine. Correlation with alar ligaments and occipito-atlantoaxial joint morphology: a examine in 50 asymptomatic subjects. Sakaura H, Hosono N, Mukai Y, Ishii T, Yoshikawa H (2003) C5 palsy after decompression surgical procedure for cervical myelopathy: review of the literature. Prospec tive correlation of magnetic resonance imaging and discography in asymptomatic subjects and ache sufferers. Shimomura Y, Hukuda S, Mizuno S (1968) Experimental examine of ischemic harm to the cervical spinal wire. Shingyouchi Y, Nagahama A, Niida M (1996) Ligamentous ossification of the cervical spine within the late middle-aged Japanese men. Terayama K, Ohtsuka K, Merlini L, Albisinni U, Gui L (1987) Ossification of the spinal liga ment. Vernon H, Mior S (1991) the Neck Disability Index: a examine of reliability and validity. Wada E, Yonenobu K, Suzuki S, Kanazawa A, Ochi T (1999) Can intramedullary signal change on magnetic resonance imaging predict surgical end result in cervical spondylotic myelopathy Correla tion of median, ulnar and posterior tibial nerve responses with clinical and radiological findings. A randomized examine, with or with out plate fixation, utilizing radiostereometry in 27 sufferers. In since antiquity 1934, Mixter and Barr had been the first to describe this correlation of their landmark paper [ninety five]. In 1939, Love [eighty four] and Semmes [122] independently developed the classic approach, which consisted of a subtotal laminectomy and retraction of the thecal sac medially to expose and take away the disc herniation [5]. Among a cohort of 2077 workers in Finland who had no sciatic ache at final analysis, 194 (9%) skilled sciatic ache throughout a 1-year comply with-up interval. Women and men had an equal threat of suffering from sciatic ache, but the incidence increased with age. A nerve root block (c)was d accomplished with an injection of corticosteroids and native anesthetics which resulted in a regression of the extreme ache inside three days. The first episode of sciatic ache was at an average age of 37 years, with precipitating low again ache in 76% of these sufferers a decade earlier [17]. A peak incidence is famous within the 4th decade with 75% of the protruded as within the lumbar spine discs occurring beneath T8. In a pc aided analysis of 2504 operations for disc spinal surgical procedure herniation, Spangfort [128] reported that the common age was forty. Five to 15-fold variations within the surgical procedure charges have been documented in variations geographically adjoining small areas, between massive areas of the United States, and in different Western nations [eleven, 34]. Pathogenesis Lumbar intervertebral disc herniation usually happens because of age-related changes within the extracellular matrix of the intervertebral disc, which may result in a weakening of the anulus fibrosus, making it vulnerable to fissuring and tear ing (see Chapter 4). Neverthe Occupational physical less, a number of occupational elements are believed to be associated with an increased elements increase the chance threat of sciatica and disc herniation: of disc herniation frequent heavy lifting [66, ninety six] frequent twisting and bending [ninety six] publicity to vibration [sixty five, 66] sedentary activity [sixty five] driving [67] A more comprehensive analysis of threat elements, however, showedthat, e. However, true traumatic disc herniation is extraordinarily rare with out addi tional extreme injuries such as vertebral fractures or ligamentous injuries [1, three, 44, 107]. In an in vitro biomechanical examine, a disc protrusion could possibly be produced as True traumatic disc a results of a hyperflexion damage [2]. We suggest being very tentative utilizing herniations are very rare the term �traumatic disc herniation� as a result of the damage regularly affects a in a clinical setting motion section which already displays age-related (degenerative) changes. The clinical syndrome of sciatica is a direct results of the impact of the disc her niation on the adjoining nerve root. This symptom could be accompanied by nerve root root pressure indicators and a sensorimotor deficit (nerve dysfunction). Innerve Nerve root compression roots exposed to significant compression, an intraneural edema developed. The results also point out that the dietary transport may be impaired at very low pressure ranges and that diffusion from adjoining tissues with a greater dietary supply, together with the cerebrospinal fluid, could not fully compensate for any compression-induced impair Figure 1. In a clinical examine on sufferers with disc herniation, Smyth and Wright [127] handed a nylon strip around the involved nerve root and brought its two ends to thesurface. It was hypothesized that chemical elements from the chromic gut play a task within the pathophysiology and growth of lumbar radiculopathy [63]. In a examine on canine, nucleus pulposus materials was applied within the epidural house and resulted in inflammatory alterations. Such mechanisms are based on the direct biochemical effects ofnucleuspulposuscomponentsonnervefiberstructureandfunction and microvascular changes together with inflammatory reactions within the nerve [106]. In subsequent studies, the identical researcher showed that the epidural application of nucleus pulposus causes proinflammatory reactions as indicated by leukotaxis and an increase in vascular permeability [one hundred], leads to an increased endone urial fluid pressure and decreased blood move within the dorsal root ganglia [154], and leads to morphologic changes when it comes to minor axonal and Schwann cell harm [28]. Clinical Presentation History Most lumbar disc herniations occur between 30 and 50 years of age. Frequently, the sufferers report an acute episode with again ache which radiates more and more into one leg inside hours or a number of days. With additional persistence of the symp toms, sufferers solely or predominantly complain of leg ache. In this younger age group, sufferers usually current with: symptom in children predominant again ache radicular or pseudoradicular leg ache hamstring tightness difficulties stooping and selecting up issues restriction in operating and leaping diminished stride Patients occasionally current with an enormous disc herniation (Case Study 1)which compresses the cauda equina, inflicting a cauda equina syndrome which is charac terized by: incapacitating again and leg ache numbness and weakness of the lower extremities incapability to urinate (early) paradoxic incontinence (later) bowel incontinence (late) Disc Herniation and Radiculopathy Chapter 18 487 Figure 2. Therefore, it der and bowel dysfunction is essential to inquire about bowel and/or bladder dysfunction. With increasing bladder distension, the sufferers develop a paradoxic incontinence caused by urinary retention. Large disc her niations that are rapidly compromising the spinal wire result in a progressive paraparesis. In sufferers in whom the compromise of the spinal wire is less extreme, prognosis is often delayed. Frequent signs indicating thoracic symp toms are: localized dorsal ache belt-like ache radiation increased ache with coughing and sneezing gait disturbance non-dermatomal sensory deficits motor weakness within the lower extremities Physical Findings the clinical examination of sufferers with radicular leg ache is predominantly focused round a neurologic examination (see Chapter eleven). A precise testing of dermatomal sensation and the muscle pressure of the lower extremities is manda tory. Patients with a herniated disc usually current with: optimistic Las`egue (straight leg elevating) sign (L4�S1) optimistic reversed Las`egue sign (L2�4) crossed Las`egue take a look at vertebral shift (Case Study 2) restricted spinal actions (non-specific) trigger points alongside the ischiadic nerve (non-specific) 488 Section Degenerative Disorders A optimistic Las`egue sign with Testing of the Las`egue sign (straight leg elevating) is essential for the prognosis of a radicular ache is indicative radiculopathy (see Chapter 8). Radicular ache have to be differentiated from non radicular leg ache, which is frequent and infrequently related to tight hamstrings.