Fulvicin
"Generic 250mg fulvicin, anti fungal supplements".
By: W. Mortis, M.B.A., M.D.
Professor, University of Michigan Medical School
The advantage of endoscopy is in the evaluation of the the orientation of a coin or other flat object gives a clue to antifungal krem vajina effective fulvicin 250mg extent and severity of the esophageal harm anti fungal wash for horses proven 250 mg fulvicin. If located in the esophagus anti fungal wash for horses generic 250 mg fulvicin, it lies in the coronal ageal perforation fungus from pedicure safe 250mg fulvicin, however, requires a very cautious method, airplane. In the acute section, ultrasound can demonstrate an elevated thickness of the pharynx wall, the proximal esophagus, and the cardia (Fig. Corrosive Esophagitis Tips from the Pro the ingestion of household cleaning products (alkalis, acids, bleaches) or burns (microwave-overheated child food) may lead the absence of mouth lesions due to a short while of contact to this condition. Acid compounds produce a coagulative necrodoes not exclude harm of the esophagus. However, some vascular anomalies may remain clinically silent, being found only incidentally. A broad variety of vascular rings and slings can occur, but the two groups of best scientific significance are these involving the aortic arch and the pulmonary artery. Chest radiography as a first-line imaging modality reveals the place of the aortic arch and any anomalies of the airways and secondary airway obstruction that could be current. Aortic Arch Anomalies Most malformations of the aortic arch may be explained by the hypothetical double aortic arch postulated by Edwards (Fig. This double aortic arch encircles the esophagus and trachea and has a ductus arteriosus on both sides. The normal, left-sided aortic arch results from regression of the proper aortic arch distal to the origin of the proper subclavian artery. Aortic arch anomalies result from failure of this regression, or regression in an abnormal website. The esophageal mucosa is markedly swollen (asterisks) and tightly surrounds the nasogastric tube (arrowheads). The aberrant subclavian artery arises from the descending aorta and may be seen in cross-section behind the esophagus (Fig. As a consequence, a right aortic arch is current from regression of the proper aortic arch distal to the origin of the proper along with a right descending aorta. Aortic arch anomalies result from failure of this vian artery arises because the final branch from a normally giant regression (double aortic arch) or regression in an abnormal website. The left-sided arch with aberrant left subclavian artery; four, right aortic arch with ductus arteriosus extends from this diverticulum to the left pulmirror-image branching. The aberrant right subclavian artery (open arrowhead)is seen in cross-section behind the esophagus. Transsternal axial scan at the level of the pulmonary artery (b) and axial scan the extent of the aortic arch. Contrast imaging of the in contrast to a right aortic arch with mirror-image branching. On contrast imaging, indentation of the rior indentation as the proper arch crosses posterior to the esophesophagus on the proper side and in addition a big posterior indentaagus to be a part of the left arch. Ultrasound Ultrasound demonstrates each arches and their widespread exhibits the proper aortic arch, no branching of the primary vessel ariscarotid and subclavian arteries on suprasternal almost sagittal ing from the aorta (left widespread carotid artery), and a big views. With slight clockwise rotation of the transducer, the left Kommerell diverticulum behind the esophagus giving rise to arch is imaged on the left side of the esophagus. A clue to the prognosis is that each arch gives rise to only two major vessels (Fig. Double Aortic Arch On a transverse scan, one will notice that the carotid and subDouble aortic arch results from the persistence of each arches. The this entire vascular ring tightly encircles the trachea and full vascular ring is displayed on a trans-sternal axial view esophagus. In a suprasternal coronal airplane, each arches are ipsilateral widespread carotid artery and subclavian artery imaged in cross-section. The right aortic arch is normally somewhat bigger in diameter and barely larger in place than the left. OccasionAnomalies of the Pulmonary Arteries: ally, a portion of the left arch is atretic. The two arches fuse into Pulmonary Artery Sling a single descending aorta, which descends on the left or less typically stays on the proper. In pulmonary artery sling or aberrant left pulmonary artery, On a chest radiograph in the anteroposterior projection, the the left pulmonary artery arises from the proper pulmonary trachea is fastened in the midline between each arches and poorly artery. To reach the left lung, it hooks around the carina and 166 Mediastinum crosses behind the trachea and in front of the esophagus (Fig. This anomaly is frequently associated with tracheobronchial malformations (lengthy segmental tracheal and left major bronchial stenosis with absence of the membranous half and full cartilage rings). Contrast imaging of the esophagus on lateral view exhibits an anterior pulsating indentation of the esophagus. Parasternal transverse ultrasound scan reveals absence of the conventional origin of the left pulmonary artery and displays the origin of the left pulmonary artery from the dorsal aspect of the proper pulmonary artery (Fig. A suprasternal scan in the airplane of the aortic arch exhibits each the proper and aberrant left pulmonary arteries in cross-section beneath the aortic arch. The barely bigger right pulmonary artery is found ventral to the smaller left pulmonary artery (Fig. Tips from the Pro the following three facts need to be proved to doc normal anatomy of the mediastinal vessels and to exclude vascular rings or a vascular sling: A left-sided aortic arch. Pulmonary sling is the one vascular anomaly that causes an anterior indentation of the esophagus. Anomalies of the Pulmonary Veins: Total Anomalous Pulmonary Venous Return Because of abnormal improvement of the widespread pulmonary vein in complete anomalous pulmonary venous return, the pulmonary veins unite posterior to the center and form a single vessel, which drains to the proper-sided circulation. According to the drainage, four kinds of lesion are described: kind I (supracardiac connection), in which the widespread pulmonary vein joins the persistent left superior vena cava on the left or the azygos Fig. The anomalous left pulmonary artery (arrowheads) arises from the proximal right pulmonary artery (asterisk) and passes between trachea (open arrowhead) and esophagus (arrow) to the left lung. The proximal right pulmonary artery and ascending aorta have almost equal diameters. Inflammatory lymphadenopathy interstitial pulmonary edema brought on by pulmonary venous is more frequent than neoplastic illness. Abdominal ultrasound will demonstrate the big adenopathy is normally brought on by viral decrease respiratory infecinfradiaphragmatic connection of the widespread pulmonary vein tion. Other widespread causes are fungal, mycoplasmal, or tuberinto the portal venous system (Fig. Noninfectious bilateral lymphadenopathy happens with sarcoidosis, Langerhans cell histiocytosis, Wegener Tips from the Pro granulomatosis, or metastatic illness. Unilateral lymphadenopathy is usually associated with major tuberculosis and is When pulmonary edema is current on a neonatal chest found frequently in mycoplasmal or fungal infections. Necrotic areas in lymph nodes are widespread in patients with tuberculosis, fungal infections, and neoplasms corresponding to ovarian carcinoma, seminoma, and rhabdomyosarcoma. Calcified lymph nodes can localization and extent of a lesion, as well as its internal strucalso be seen in sure malignancies, corresponding to osteosarcoma, ture and vascularity. Ultrasound has a screening function in the mucinous ovarian carcinoma, and papillary carcinoma of the evaluation of mediastinal masses. Compartmentalization of the mediastinum is helpful in Chest radiography is the primary-line imaging modality, and producing a possible dierential prognosis. Mediastinal sonography has additionally proved to be a priceless the compartment in which they typically arise. Benign thymic device in demonstrating mediastinal lymph node enlargement in enlargement, malignant lymphoma, teratomas, foregut cysts, children. Solitary or a number of enlarged lymph nodes or a stable and neurogenic tumors account for eighty% of mediastinal masses mass representing the coalescence of a number of nodes may be in children. Enlargement of the left vertical vein (open arrowheads) and right superior vena cava (arrowheads) results in the typical figure-of-eight appearance (�snowman heart�). Both lung fields show diffuse reticular vascularity, attribute of passive vascular engorgement. Longitudinal (b) and axial (c) scans by way of the higher abdomen show the big widespread pulmonary vein (arrows) crossing the diaphragm and draining instantly into the portal vein (open arrows). Mediastinal nodal involveTips from the Pro ment is seen in 85% of circumstances and hilar adenopathy in 25%. Dis Mediastinal lymph nodes are greatest detected with small transcrete nodular masses or confluent homogeneous or heterogeducers from the supraclavicular or suprasternal method. Frequently, involvement of hilar, subIn children and adolescents, lymphoma is the commonest carinal, posterior mediastinal, and paracardiac nodes is proven.
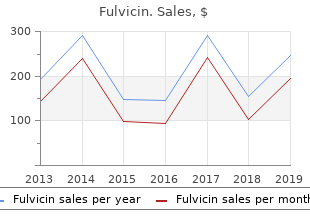
For score=02 (N=236) (open box) antifungal medication side effects 250 mg fulvicin, the median survival was fifty six months and the 5year survival 47% fungus gnats water effective fulvicin 250 mg. For score =34 (N=fifty seven) (stuffed triangles) fungi phylum trusted fulvicin 250 mg, the median survival was 32 months and the 5-yr survival 24% fungal nail salon cheap 250 mg fulvicin. Using one point for each criterion, a summed score of 02 puts sufferers in a low threat group and is a powerful indication for hepatectomy. In these high threat sufferers, a period of statement with no therapy or systemic chemotherapy permitting for the extent of metastases to declare themselves is affordable. Neuroendocrine tumors Patients with symptomatic neuroendocrine tumors ought to be considered for resection or ablation. For the small tumor, signs are most probably derived from hormonal secretion by the tumors, and such hormone ranges may also present a marker for effectiveness of the ablation or resection. For asymptomatic tumors, a period of statement to enable evaluation of the tempo and aggressiveness of the tumors is affordable when the tumors are small. The prognostic factors of significance on multivariate evaluation included the disease-free interval (>36 months), healing resection (versus palliative incomplete resection) and first tumor kind. Their conclusions would recommend that regardless of histology, with a protracted disease-free interval sufferers could profit from surgical resection. Resection strategies For small solitary metastases to the liver, the objective of resection is to completely excise the tumor whereas preserving the maximum regular hepatic parenchyma. Preserving parenchyma facilitates postoperative restoration and in addition offers flexibility for additional resections should intrahepatic recurrences occur. Even for wedge resections, ultrasound is helpful in defining the vascular anatomy around the lesion, which may help decrease blood loss. Wedge resections Wedge resections must be carried out meticulously to keep away from inadvertently leaving a Surgical management of hepatobiliary and pancreatic disorders 134 constructive margin. Large chromic liver sutures can be placed and used for retraction during dissection. The parenchymal dissection ought to be carried out along the lines used for different forms of liver resection. We prefer the Kelly clamp method where the clamp is used to crush the traditional parenchyma, exposing vessels which are then clipped, tied, suture ligated or stapled utilizing a vascular stapling system. This method is superior to the straightforward use of electrocautery for the dissection which is usually tried for what appears to be routine wedge resections. The char effect of the electrocautery prevents enough visualization of the anatomy, making it quite easy to stray into massive vessels or into the tumor. The most tough margin in performing a wedge resection is the deep margin of dissection. Using intraoperative ultrasound, the depth of dissection ought to be measured prior to the initiation of parenchymal dissection, together with no less than a 1 cm margin deep to the tumor. The dissection ought to be carried down perpendicular to the liver surface to the predetermined depth. At this point the tumor can be lifted up and dissection can proceed horizontally throughout the bottom of the wedge. The tendency to resect with a �V-formed method� is more likely to be difficult by a constructive deep margin. At the top of the dissection the Pringle maneuver is eliminated and the argon beam coagulator is used to management bleeding vessels. Careful examination is made for any proof of a bile leak, which is managed with suture ligature. When the zone of freezing is confirmed by ultrasound to be no less than 1 cm past the tumor, wedge resection is carried out utilizing the freeze margin as the margin of resection. The cryotherapy probe makes a ready retracting system and the parenchyma is often easy to dissect on the margin of the ice-ball. Segmental resections For all but probably the most superficial lesions, we prefer a segmental method for the resection of tumor. The intersegmental planes can be identified intraoperatively utilizing vascular landmarks with the aid of intraoperative ultrasound. Using these planes for parenchymal dissection will decrease blood loss and help ensure a safe margin. Inflow occlusion for the segment can nearly all the time be carried out first, thereby producing demarcation of the segmental planes to additional enhance the dissection. The anterior sectoral pedicle can be dissected from an inferior or anterior method. The main hepatic veins lie inside the intersegmental planes, and is usually a source of serious blood loss in the course of the parenchymal transection phase of a segmentectomy. The use of low central venous stress (zero�5 mmHg) during parenchymal dissection can decrease back bleeding in these veins. When the solitary metastases lies close to an intersegmental plane, two segments can be eliminated. The caudate lobe (segment I) can be resected as an isolated segmentectomy when the tumor is confined to this lobe. The intersegmental planes were then marked by electrocautery and a proper segmentectomy was carried out with negative margins. While an aggressive resection was indicated and carried out, the affected person can nonetheless undergo a proper left or proper hepatic lobectomy in the future if indicated. Morbidity and mortality the mortality rates for main hepatic resection have decreased significantly over time to a standard reporting of mortality in the 1�four% range. In a recent report of 270 wedge or segmental resections, the operative mortality was zero. While mortality rates are low, the complication price for main hepatic resection continues to be comparatively high, ranging from 20% to 50%. They present perfect options to laparotomy and main liver resection for the treatment of small solitary hepatic metastases, for the reason that small tumor is the most probably to be completely handled by ablation strategies. Percutaneous approaches to tumor ablation are even more enticing than laparoscopic procedures. Because the affected person will probably start to fail in multiple websites in the close to future with limited survival potential, a laparotomy and hepatic resection was not considered cheap. She was handled with Surgical management of hepatobiliary and pancreatic disorders 138 percutaneous radiofrequency ablation, reaching a good zone of necrosis encompassing the mass, and she spent solely at some point in the hospital with very minimal discomfort. How such procedures, which have low morbidity and which maintain high quality of life, will issue in the treatment of sufferers with small hepatic metastases must be addressed by studies with enough observe-as much as define the native recurrence price. Even for hepatic colorectal metastases, that are generally handled with surgery, data on adjuvant chemotherapy after liver resection is sparse. There are at present no data to assist the usage of irinotecan and oxaliplatin in an adjuvant setting, though studies are in progress. For sufferers with hepatic colorectal metastases, the commonest website of tumor recurrence after liver resection is the remnant liver. Regional chemotherapy to treat the liver website is therefore a theoretically enticing option for adjuvant care. Although no difference was found between the teams, technical factors compromised this research such that solely 34 of the 114 sufferers randomized to chemotherapy completed the adjuvant remedies. For non-colorectal, non-neuroendocrine histologies metastatic to the liver probably the most Surgical management of hepatobiliary and pancreatic disorders a hundred and forty probably explanation for dying might be associated to the disease outside the liver, regardless of how the liver is managed. If the tumor responds then a resection might be carried out with confidence that different micrometastatic disease could also be effectively handled with chemotherapy. If the affected person advances systemically during chemotherapy then it is rather unlikely that a resection would have been of profit and the affected person may have averted the potential morbidity, pain, discomfort and restoration time of an hepatic resection. Conclusions Algorithms for the management of small solitary hepatic metastases are proven in Figure 6. Both affected person and tumor traits must be considered in making management choices. Immediate ablation or resection ought to be carried out in the setting of a medical trial, and most appropriately a trial inspecting adjuvant therapy. At resection, the precept ought to be to go away as much regular liver behind so as to decrease the danger of liver failure and so as to enable for repeat anatomic liver resections in the future for recurrent disease. Enucleation with constructive margins is suitable for treatment of this histology as a result of resection is nearly by no means healing, and such cytoreduction can present significant and sturdy palliation with minimal threat. For sufferers with small, solitary, non-colorectal non-neuroendocrine tumors probably the most significant issue in terms of prognosis appears to be the diseasefree interval (Fig.
250 mg fulvicin. Top 5 Dog Yeast Infection Treatment [2018 Best Sellers]: SynergyLabs Veterinary Formula Clinical.
Encasement of mediastinal structures and infiltration of quent dural cord compression fungi definition yahoo answers effective fulvicin 250 mg. Displacement of the trachea and option to antifungal shampoo for cats quality fulvicin 250mg consider the full extent of a mass fungus roots 250mg fulvicin, particularly extradural esophagus and the compression of adjacent structures occur fungus za kichwa order fulvicin 250 mg. Sudden increase in size as a result of hemorrhage or an infection may lead to a mass eect that can be life-threatening. Cystic lymphatic malformations are subdivided into macro Intraspinal extension should be detected preoperatively. On ultrasound, macrocysThink of ultrasound of the spinal cord in newborns with tic lymphangiomas are multiloculate or septate lots that neuroblastoma! In addition to bilateral widening of the mediastinum by the thymus (arrowheads), a posterior mediastinal mass (arrow) displaces the trachea (ventilation tube) and esophagus (feeding tube) to the left (open arrowhead). The central echogenic space and punctate echogenic foci (open arrowheads) represent calcifications. Ultrasound analysis after catheter elimination may show the left-behind fibrin sheath mimthe insertion of a venous catheter is associated with each icking a catheter fragment (Fig. The quick comcan be used to reveal the shortage of jet move in an obstructed plications embody catheter malposition, extraluminal placecatheter and the shortage of blood move in an obstructed vessel. Late Tips from the Pro problems are occlusion, thrombosis, sepsis, and catheter tip migration. Catheter tip migration may lead to pericardial Any chest X-ray that reveals an uncommon catheter position eusion, cardiac tamponade, or hydrothorax (Fig. Thrombosis of the superior vena suspicion if an acute pleural assortment is seen on the same cava may lead to lymphatic duct blockage and subsequently facet as the catheter. Right parasternal longitudinal scan reveals remaining fibrin sheath (arrowheads) of a catheter in the superior vena cava (arrows) after elimination of a central venous line. Trans-sternal excessive (d) and low (e) axial scans show a big quantity of echo-free pericardial effusion (asterisks) associated to catheter tip migration in the proper atrium with subsequent fluid leakage. Neuroblastoma, ganglioneuroblasRecommended Readings toma, and ganglioneuroma: radiologic-pathologic correlation. Rings, slings, and other issues: vascular compression of the infant tragenol 1992; 158: 825�832 chea up to date from the midcentury to the millennium�the legacy of Robert E. Radiology 2000; 216: 624�632 bronchial cartilaginous rings: warfarin sodium-induced calcification. The thymus: a Dis Child Fetal Neonatal Ed 2004; 89: F504�F508 comprehensive evaluate. The biology and management of subglottic hemHepatol 2011; 5: 637�645 angioma: past, current, future. Hemangiomas Chest Imaging, Berlin, Germany: Springer; 2007:1�36 revisited: the useful, the weird and the new. Sonographic analysis of oesophageal atresia and tracheorevisited: the useful, the weird and the new. Radiol Clin North dren after mitral valve replacement and warfarin sodium therapy. Radiographics 2000; 20: 653�671 Yonehara Y, Nakatsuka T, Ichioka S, Sasaki N, Kobayashi T. Aberrant thymus in infants: Craniofac Surg 2002; thirteen: 623�626 sonographic analysis. Intrathoracic vasaccessibility and bedside capabilities, which makes it a patientcular structures such as the aorta, pulmonary arteries, and friendly approach that can readily be utilized in emergency situaveins can be only superficially examined. Furthermore, it permits direct intervenevaluation of superficial structures and pleural eusions. B-mode ultraSince the final practice is that cardiac ultrasonography is sound is mostly used, in grey-scale and Doppler imaging. Ultrasound reveals an uneven aspect of the cartilage on the costosternal junction without any signs of pathology. Unossified cartilage is hypoethese instances, the findings at bodily examination can be correchoic, with variation in shape and size. Ultrasound is an eassuperficially accessible, as only the cortex can be assessed. Challenging a small youngster to maintain his or her breath as if swimming underneath water can be helpful. Ultrasound reveals the swelling to be primarily based on a prominent xiphoid (open arrowhead). The use of twin-screen imaging during which either side can be visualized facet by facet can be helpful. Ultrasound can, however, depict pleural thickbreathing, it will transfer (�gliding signal�)(Video 7. Under normal circumstances, the pleural cavity may comprise a small quantity of pattern generally known as �seashore signal� (Fig. In case of pulmonary consolidation fluid of as much as 200mL, ultrasound can simply detect them. The presence of air will cause a hyperechoic reflecrole in the imaging of pediatric breast lesions because of the tive floor with reverberation and comet tail artifacts denseness of the mammary glands and using radiation. One can appreciate the motion After birth, breasts can be enlarged in each girls and boys up of lung and visceral pleura along the parietal pleura on inspirato the age of 12 months underneath the influence of maternal hortion, the �gliding signal. In prepubertal youngsters, the breast is a group choic retroareolar tissue to fully developed breast tissue with of simple, branched, epithelium-lined ducts surrounded by conechogenic fibroglandular tissue, hypoechoic ducts, Cooper liganective tissue. Physiologic breast growth in ladies occurs between 9 and Changes in hormonal ranges can lead to uneven breast thirteen years of age underneath hormonal stimulation. Ultrasound is usually used to exclude pathology be divided in five Tanner phases ranging from delicate hypere(Fig. Ultrasound can be utilized for each Poland Syndrome anatomical and functional analysis. Features embody hypoplasia of the breast, nipples, common anatomical variant is the diaphragmatic slip. This is and subcutaneous tissue; lack of the pectoralis main muscle and characterised by a slip or fold of muscle of the diaphragm, minor musculature; and aplasia or deformity of the costal cartiwhich can cause a clean indentation of the liver or spleen. In addition, a part of Also, nodular crura and hypertrophy of the medial and lateral the syndrome can be alopecia of the axillary and mammary arcuate ligaments can be seen. A possithe motion of the diaphragm can be analyzed with ble explanation for this syndrome could also be developmental abnormality M-mode (Fig. The clinical manifestations can this technique two acoustic home windows are used, indirect transrange from aplasia of the pectoral muscular tissues alone to the entire verse subxiphoidal and intercostal. On ultrasound, an asymmetry of the chest strikes toward the transducer, and on expiration motion is because of hypoplasia or aplasia of the musculature ought to elevate the cephalad, away from the probe. Movement should be reported as both normal, absent, or Rib Anomalies paradoxical. Normal motion of the diaphragm is over 4mm Asymptomatic swelling and asymmetry of the chest will usually on M-mode, and there should be lower than a 50% dierence in be as a result of an abnormal growth of ribs, particularly of the excursion between the 2 hemidiaphragms. In these patients, chest radiographs will usually be requested by the referring physicians. However, for the reason that asymmetry is most frequently positioned in the cartilaginous a part of the rib cage, thoracic ultrasound should be the imaging methodology of Tips from the Pro first choice. Also, for the clinician, this is readily interpretable show developmental abnormalities of the cartilage and ribs information. A heterogeneous mass with hypervascularity can be seen on Doppler ultrasound with infiltration of the encircling fats. In case of a chest wall abscess, ultrasound will show an encapsulated, hypoechoic, typically heterogeneous mass. Abscess formation also can occur round surgically implanted materials corresponding to a Nuss bar (Fig. In the majority of youngsters, the presenting symptom is ache, and discoloration is visible in 50% of reported patients. Generally, laboratory examinations are normal, and microbiologic cultures are negative in all reported instances. Ultrasound reveals a well outlined, dumbbell-formed, hypoechoic, heterogeneous, poorly Fig. The lesion has no contact with reveals absence of the pectoralis main muscle on the left (evaluate a with b).
When metastatic lesions are discovered in the liver fungus gnats killer uk proven 250mg fulvicin, they need to be resected when technically possible to antifungal ointment for lips best fulvicin 250 mg restrict the signs of the carcinoid syndrome fungus gnats diatomaceous earth generic fulvicin 250 mg. Resection of the appendix and cecum could also be performed to fungal zygomycosis effective fulvicin 250 mg stop an early intestinal obstruction by locally encroaching tumor instead of a proper hemicolectomy in sufferers with liver metastasis. Patients with familial breast most cancers (multiple firstdegree relations and penetrance of breast most cancers by way of several familial generations) have extremely excessive risks of creating breast most cancers in the middle of their lifetimes. A patient with a history of familial breast most cancers and multiple biopsies displaying atypia might fairly request bilateral prophylactic simple mastectomies. Lobular carcinoma in situ is a histologic marker that identifies sufferers at increased risk for the development of breast most cancers. As the risk for the longer term development of breast most cancers is now estimated to be roughly 1% per 12 months, prophylactic mastectomy is now not really helpful. Proper administration consists of shut surveillance for most cancers by twice-yearly examinations and yearly mammography. It is described in 4 histologic variants (papillary, cribriform, stable, and comedo), of which the comedo subtype shows the best tendency to recur after broad excision alone. Omeprazole is added to the H antagonists as a therapeutic approach to the administration of acute2 gastric and duodenal ulcers. A 35-12 months-old woman presents with frequent and multiple areas of cutaneous ecchymosis. Workup demonstrates a platelet rely of 15,000/L, evaluation of the bone marrow reveals a traditional number of megakaryocytes, and ultrasound examination demonstrates a traditional-sized spleen. Immediate platelet transfusion to improve platelet counts to higher than 50,000/L c. A fifty nine-12 months-old woman presents with proper lower quadrant pain, nausea, and vomiting. Manometry shows a hypertensive lower esophageal sphincter with failure to loosen up with deglutition. Which of the following is the most secure and handiest remedy of this situation Medical remedy with sublingual nitroglycerin, nitrates, or calcium-channel blockers b. Which of the following is essentially the most acceptable elective operation for this patient Total proctocolectomy with ileal pouch-anal anastomosis and diverting ileostomy c. Total proctocolectomy with ileal pouch-anal anastomosis, anal mucosectomy, and diverting ileostomy d. A 39-12 months-old previously healthy male is hospitalized for 2 weeks with epigastric pain radiating to his back, nausea, and vomiting. Initial laboratory values revealed an elevated amylase stage consistent with acute pancreatitis. Five weeks following discharge, he complains of early satiety, epigastric pain, and fevers. Which of the following can be essentially the most definitive administration of the fluid assortment Surgical inside drainage of the fluid assortment with a cyst-gastrostomy or Roux-en-Y cystjejunostomy 297. A previously healthy 79-12 months-old woman presents with early satiety and belly fullness. A 56-12 months-old woman is referred to you about three months after a colostomy subsequent to a sigmoid resection for most cancers. Which of the following is the most common severe complication of an end colostomy A 56-12 months-old previously healthy doctor notices that his eyes are yellow and he has been shedding weight. On physical examination the patient has jaundice and scleral icterus with a benign abdomen. Transcutaneous ultrasound of the abdomen demonstrates biliary ductal dilation without gallstones. Which of the following is essentially the most acceptable subsequent step in the workup of this patient A 45-12 months-old woman with history of heavy nonsteroidal anti-inflammatory drug ingestion presents with acute belly pain. She undergoes exploratory laparotomy 30 hours after onset of signs and is discovered to have a perforated duodenal ulcer. Six weeks after surgical procedure, he returns, complaining of postprandial weakness, sweating, gentle-headedness, crampy belly pain, and diarrhea. Dietary advice and counseling that signs will most likely abate within three months of surgical procedure c. A 60-12 months-old male patient with hepatitis C with a earlier history of variceal bleeding is admitted to the hospital with hematemesis. His blood strain is eighty/60 mm Hg, physical examination reveals splenomegaly and ascites, and initial hematocrit is 25%. Prior to endoscopy, which of the following is the most effective initial administration of the patient A 32-12 months-old alcoholic with end-stage liver disease has been admitted to the hospital three occasions for bleeding esophageal varices. Which of the following is the most suitable choice for lengthy-term administration of this patient�s esophageal varices A 45-12 months-old man was found to have a hepatic flexure colon most cancers during a colonoscopy for anemia requiring transfusions. Upon exploration of his abdomen in the operating room, an sudden discontinuous three-cm metastasis is found in the edge of the right lobe of the liver. Preoperatively, the patient was endorsed of this risk and the surgical choices. Which of the following tests supplies the least invasive methodology to doc eradication of the infection Which of the following hernias follows the trail of the spermatic cord inside the cremaster muscle An eighty-12 months-old man with history of symptomatic cholelithiasis presents with indicators and signs of a small-bowel obstruction. Which of the following findings would supply essentially the most assist in ascertaining the diagnosis A forty two-12 months-old man has bouts of intermittent crampy belly pain and rectal bleeding. The patient is successfully handled by removing as many polyps as attainable with the help of intraoperative endoscopy and polypectomy. A 70-12 months-old woman has nausea, vomiting, belly distention, and episodic crampy midabdominal pain. She has no history of earlier surgical procedure however has a long history of cholelithiasis for which she has refused surgical procedure. Which of the following is the definitive remedy for this patient�s bowel obstruction A fifty three-12 months-old man presents to the emergency room with left lower quadrant pain, fever, and vomiting. After percutaneous drainage and remedy with antibiotics, the pain and fluid assortment resolve. He undergoes a colonoscopy, which demonstrates solely diverticula in the sigmoid colon. A 29-12 months-old woman complains of postprandial proper upper quadrant pain and fatty meals intolerance. Upper endoscopy is normal, and all of her liver perform tests are within normal limits. Ultrasound examination ought to be repeated immediately, for the reason that falsenegative fee for ultrasound in detecting gallstones is 10% to 15%. A forty seven-12 months-old asymptomatic woman is incidentally discovered to have a 5-mm polyp and no stones in her gallbladder on ultrasound examination. Observation with repeat ultrasound examinations to evaluate for improve in polyp size c. En bloc resection of the gallbladder, wedge resection of the liver, and portal lymphadenectomy 314. A forty eight-12 months-old woman develops pain in the right lower quadrant whereas enjoying tennis.